

COVID news & more 1/6/2024

It is time to put on an N95 or KN95 mask and get vaccinated (vaccines.gov for appointments) if you haven’t already. Adults can get free antiviral medication like Paxlovid for COVID infections or Tamiflu for the flu, whether or not they have health insurance at Test2Treat.org. If you sign up in advance before an infection, Test2Treat.org will also send you free COVID tests.
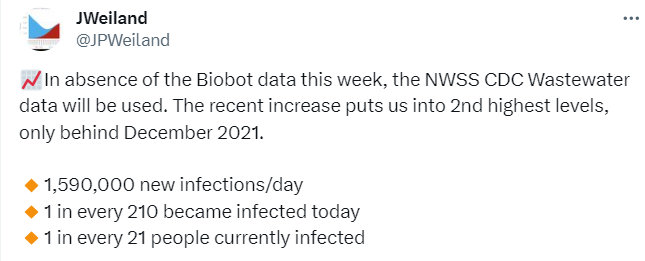
JP Weiland estimates that 1 in 21 people in the United States has COVID now and there are 1.6 Million new COVID infections every day. That number is expected to go to up to 2.0 million people being infected with COVID every day within the next week or two. It is not just the height of the peak of COVID infections (number of daily infections) in a wave that is important. The total area under the curve (i.e. both the height and the width of the wave in days) will affect the total number of people infected in that wave. It is estimated that about 1 in 3 Americans will be infected during this wave which translates to 100 million people who will be infected.
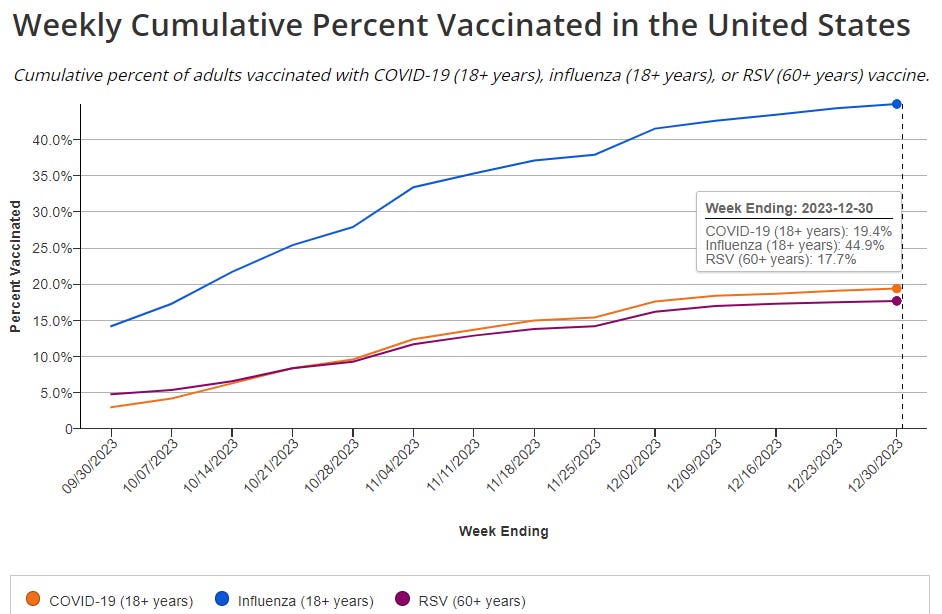
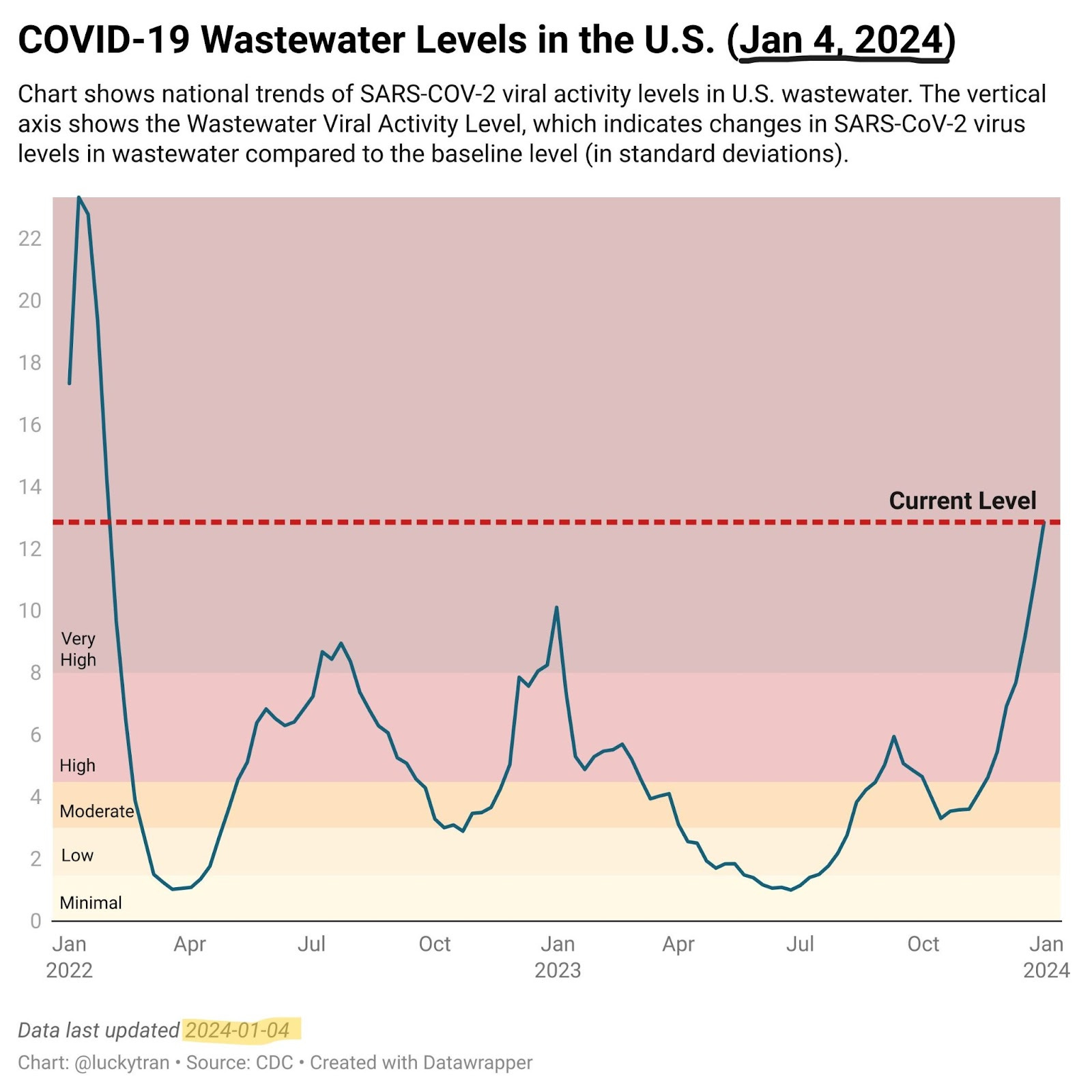
The Pirola variant JN.1 has taken off in the United States and is now responsible for 62% of COVID cases nationally. This tracks with JN.1 exploding in many countries around the world. In the U.S., COVID hospitalizations are up 20.4% this week and emergency room visits for COVID are up 13%. Only 19.4% of American adults have received the updated XBB.1.5 COVID vaccine. Protection from prior vaccines does not last more than about 4 to 6 months. It is important to get the updated vaccine if you have not yet. We are in the 2nd largest COVID wave since the beginning of the pandemic four years ago and it is time to take precautions.

Influenza is also high now and is causing hospital admissions and emergency room visits in addition to COVID admissions. In Italy, the hospitals are completely overwhelmed with sick patients with influenza and with COVID. More than 1,100 patients were reported to be waiting to be admitted to hospitals in Rome. Italian politicians complained of "blocked ambulances, postponed operations, clogged emergency rooms and beds blocked by COVID patients, all because of a vaccination campaign that started late". Here in the U.S., Dr. Kaminski from Yale recently posted that Yale had 3x more hospitalized COVID patients compared to Flu or RSV, and the numbers for COVID had increased significantly in the last few days. He stated “[I’m] not aiming to spread panic, simply [trying to] inject reality, advocate caution, updated vaccines and masking up where appropriate.”
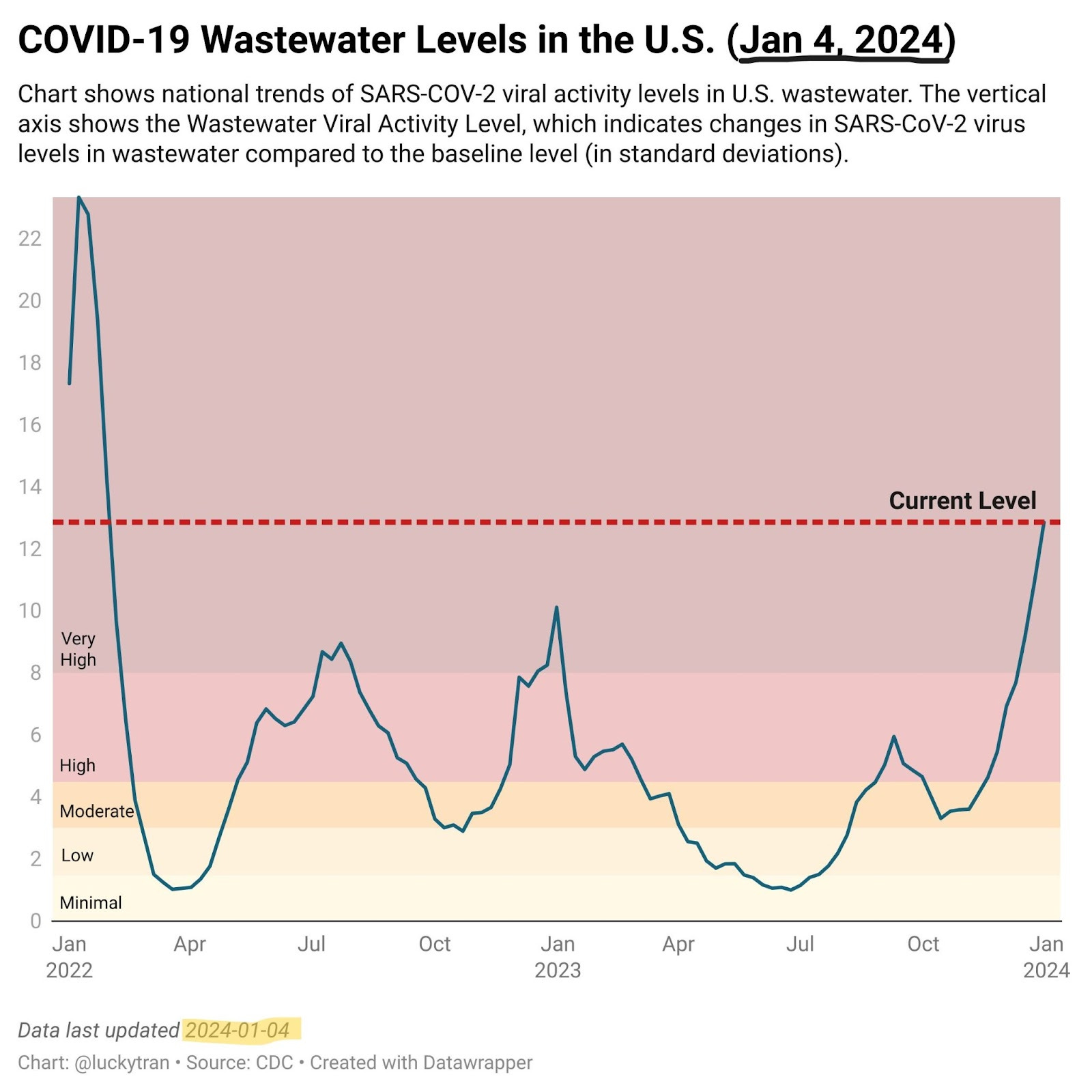
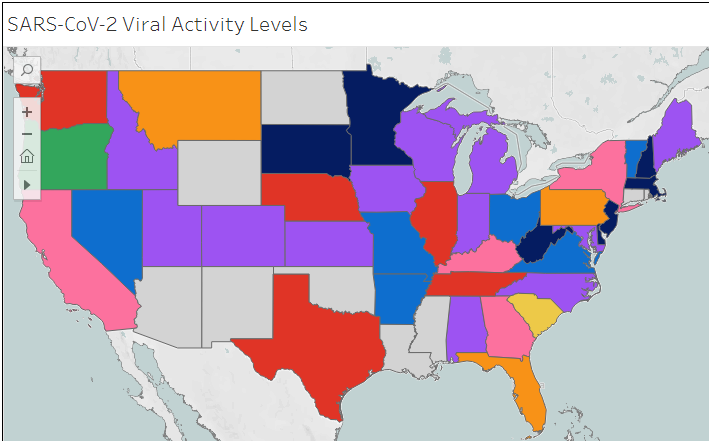
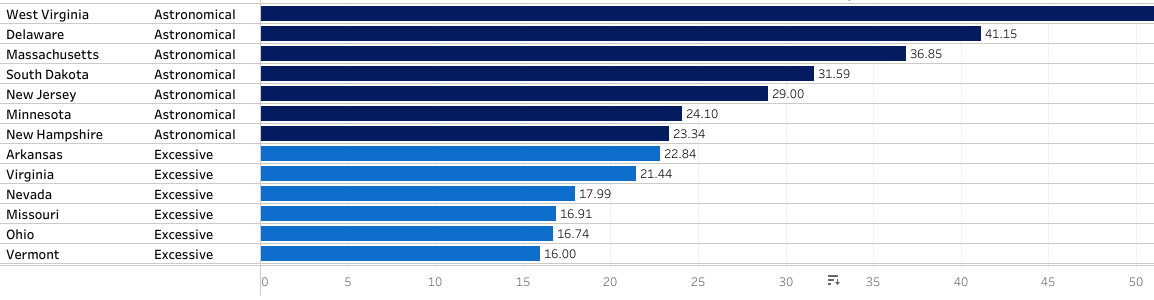
U.S. wastewater levels of SARS-CoV-2 are “VERY HIGH” this week per the CDC. Wastewater levels of COVID are continuing to increase and are at their highest levels since the Omicron wave in 2021-2022. I recently found national SARS-CoV-2 data from Sarah Anne Willette on her website https://iowacovid19tracker.org/. She lives in Iowa, but tracks COVID across the U.S. and Canada. She reports that SARS-CoV-2 virus levels are “astronomical” in several states including West Virginia, Delaware, Massachusetts, South Dakota, New Jersey, Minnesota and New Hampshire. Looking at the numbers, I think that “astronomical” is an appropriate description.
A OpEd by Eric Topol MD in the Los Angeles Times yesterday asks, “The U.S. is facing the biggest COVID wave since Omicron. Why are we still playing make-believe?” He says, “"Now in its fifth year, SARS-CoV-2 has once again proved to be highly resilient, capable of reinventing itself to infect us. Yet we continue to make-believe that the pandemic is over, that infections have been transformed to common cold status by prior exposure(s), and that life has returned to normal. Sadly, none of this is true.” With massive numbers of COVID infections (remember, we are at 1.6 Million new infections every day now), there will be massive numbers of people getting Long COVID which will cause massive disability. Dr. Topol also discussed that for older people, those who are immunocompromised and those with chronic conditions, getting a COVID infection is not like getting a cold- it can be much worse.
Pediatrics
A new article in the Journal of Pediatrics shows that one-third of infants hospitalized with a COVID infection had elevated Troponin levels and that the youngest babies had the highest risk. Troponin is a blood test that shows when there has been damage to the heart muscle. For instance, when someone has a heart attack, their troponin levels rise. Although the Troponin elevations in the babies hospitalized with COVID were transient and resolved after they were discharged home, long-term consequences to their hearts are unknown. As Raina MacIntyre tweeted, “Imagine the effect [of possible transient heart damage] on a generation of infants and children subject to repeated infections.”
It is true. We do not know the long term effects of children being reinfected with COVID. We do know, at least in adults, that repeated COVID infections increase the risk of Long COVID. In July 2023, a review of 31 studies in the journal Pediatrics showed that 1 in 6 children and teens do not fully recover from COVID infection. At 3 months, 16% of kids have lingering symptoms. And while sore throat, fever, and sleep disturbance were the most common symptoms, some children have a more disabling type of Long COVID.
Schools are now back in session. We are in a huge COVID wave with at least 1.6 million new cases of COVID each day and that is expected to increase to 2.0 million new daily COVID cases in the U.S. within the next week or two. More than 70% of US household COVID spread starts with a child, especially when school is in session. Reducing childhood COVID infections benefits the whole family, including the child. Mike Hoerger wrote this letter for parents and schools regarding the need for better ventilation and other mitigations in schools.
Vaccines
A well-written article in Scientific American reviewed studies showing that COVID vaccination dramatically lowers the risk of Long COVID. Protection against Long COVID was found to be dose dependent in several studies. A study from Sweden of almost 600,000 people showed that receiving 1 dose of COVID vaccine reduced the risk of Long COVID by 21%, 2 doses of COVID vaccine reduced the risk of Long COVID by 59% and 3 doses of a COVID vaccine reduced the risk of Long COVID by 73%. Similar findings were seen in a meta-analysis of 24 other studies.
A preprint article that I reported on last week co-authored by Kaiser Permanente Southern California and Pfizer may have been misleading. The authors concluded: “XBB1.5-adapted vaccines provided significant additional protection against a range of COVID-19 outcomes and older versions of COVID-19 vaccines offered little, if any, additional protection, including against hospital admission, regardless of the number or type of prior doses received.” But that isn't really what the data shows. Michael Mina tweeted that these researchers were comparing the new XBB.1.5 Pfizer vaccine to older versions of COVID vaccines that were given about a year ago. Older versions of the COVID vaccine may not be as effective now because they were given a year ago and people’s immunity from them had waned. He points out that one cannot assume that the older vaccines would not protect against today’s variants if they are not given anymore. Still, we are fortunate that several studies have shown that the new XBB.1.5 updated COVID vaccines protect against variants like JN.1 that are in circulation now.
A few days ago, the Florida Surgeon General Dr. Ladapo released a statement saying that COVID mRNA vaccines may not be safe and that the FDA didn’t answer his questions, so he recommended stopping the use of all COVID mRNA vaccines. The FDA responded, "The FDA stands firmly behind the safety, effectiveness and manufacturing quality of the approved and authorized COVID-19 vaccines, and respectfully disagrees with the Florida Surgeon General’s opinion.” "With over a billion doses of the mRNA vaccines administered, no safety concerns related to residual DNA have been identified." Katelyn Jetelina and colleagues responded to Dr. Ladapo’s claims with “7 pieces of context missed from Florida Surgeon General’s unnecessary warning.”
Long COVID
Why can’t people with the ME/CFS-type of Long COVID exercise? It turns out that their muscles are abnormal as seen by a new landmark study from Rob Wust’s lab in the Netherlands. In Long COVID, the mitochondria that make the energy for muscle cells no longer work correctly. Exercise actually also causes severe muscle damage and even muscle necrosis in people with Long COVID. There are also structural changes in skeletal muscles in Long COVID including an increase in glycolytic muscle fibers that tire very easily, mitochondria that cannot make energy in the normal way, and increased amounts of amyloid deposits in between skeletal muscle fibers. All of these abnormalities also contribute to post-exertional malaise (PEM) in Long COVID. PEM can cause muscle pain, weakness, exhaustion and even a feeling of “being poisoned”. This study shows that exercise can be toxic for people with ME/CFS-type Long COVID because of the above skeletal muscle abnormalities.
What is amyloid anyway? Amyloid deposits contain proteins made of peptides that can form a repetitive β-sheet fibrillar structure. Amyloid deposits are seen in the brains of Alzheimer patients and Parkinson’s patients (alpha-synuclein) and in the hearts of people with cardiomyopathy. C-reactive protein (CRP) is an amyloid protein with antimicrobial properties. Amyloid is associated with inflammation and may be a part of our innate immunity. Amyloid deposits are made of protein that is clumped together with polyanionic substances like nucleic acids and polysaccharides.
Rob Wust’s lab found impaired peripheral oxygen extraction in people with Long COVID as other studies have shown. Amyloid deposits were found to be located in between muscle fibers of people with Long COVID, but amyloid did not block capillaries. After exercise, the amount of amyloid deposits increased in the muscles of LC patients. The authors also found that in Long COVID, there is more muscle atrophy, muscle necrosis, internal nuclei (muscle fiber repair), muscle fiber regeneration, CD3+ T cell infiltration and more infiltration by CD68+ macrophages (see Figure 5). In addition, large areas of necrotic muscle fibers (dead tissue) were found in 36% of patients with long COVID after exhaustive exercise. Yikes!
In a tweet thread explaining the article, Rob Wust mentioned that it took a while for the paper to be reviewed and edited before being published. During that time, his lab has continued to work on understanding how to reduce PEM in Long COVID. “Stay tuned!” he tweeted.
A new review article written by specialists from Sweden, Austria, Canada, United States, and the UK looked at Cardiovascular Autonomic Dysfunction (CVAD) in Long COVID. While POTS and inappropriate sinus tachycardia were the most common symptoms in Long COVID, CVAD can also lead to microvascular and endothelial cell dysfunction which can lead to headaches, brain fog, and peripheral circulatory symptoms like heat and cold intolerance, Raynaud-like symptoms and skin discoloration. Authors concluded that both non-pharmacologic (exercise training, blood volume expansion and compression garments) and medications that target heart rate, blood volume expansion, vasoconstriction and venoconstriction, and reduction of hyperadrenergic drive can be helpful.
Twins were featured in two different non-COVID news stories this week. Twin boys Ezra and Ezekiel were born on two different days in two different years! Baby Ezra arrived Dec 31, 2023 at 11:48 pm and his brother Ezekiel was born on Jan 1, 2024 at 00:28 am.
Earlier in December, a woman with two uteruses, a condition called uterus didelphys, had twin baby girls also born on two different days. The babies were rare dicavitary twins meaning that one baby grew in the right uterus and the other baby in the left uterus. Baby Roxi delivered vaginally on December 19 and her sister Rebel had to be delivered by c-section 10 hours later on December 20. They are all doing well.
Have a good rest of your weekend,
Ruth Ann Crystal MD
COVID news:
US Variant tracker: https://covid.cdc.gov/covid-data-tracker/#variant-proportions



CDC COVID data tracker: https://covid.cdc.gov/covid-data-tracker/index.html#datatracker-home

CDC COVID Hospitalizations (blue) and Emergency Room (orange) visits tracker: https://covid.cdc.gov/covid-data-tracker/index.html#trends_weeklyhospitaladmissions_7dayeddiagnosed_00

Weekly ED visits for respiratory illnesses, by age and disease: https://www.cdc.gov/ncird/surveillance/respiratory-illnesses/index.html




US Wastewater Monitoring:
CDC wastewater reporting: https://www.cdc.gov/nwss/rv/COVID19-nationaltrend.html


CDC wastewater map: https://www.cdc.gov/nwss/rv/COVID19-currentlevels.html


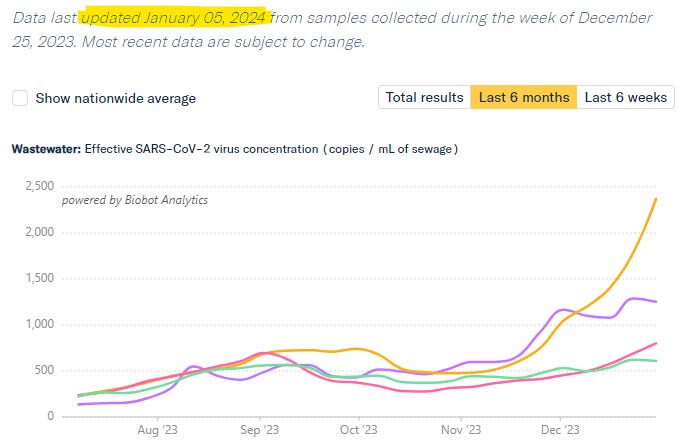
Biobot: https://biobot.io/data/
National SARS-CoV-2 data from Sarah Anne Willette: https://iowacovid19tracker.org/

Viral activity, week of December 23, 2023
Wastewater SCAN: https://data.wastewaterscan.org/
Sewer Coronavirus Alert Network (SCAN) project by Stanford University:


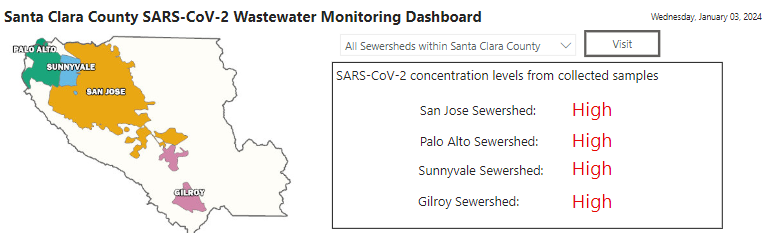
Santa Clara County wastewater: https://covid19.sccgov.org/dashboard-wastewater
CDC Respiratory vaccination trends: https://www.cdc.gov/respiratory-viruses/data-research/dashboard/vaccination-trends-adults.html
Adults 18+
COVID vaccine: 19.4%
Flu shot: 44.9%
RSV (60+): 17.7%
JP Weiland: https://twitter.com/JPWeiland

1/5/24 Today: A viral social media post claims 1 in 3 people will get COVID this winter. Is it true? https://buff.ly/4aNzsLa
Lucky Tran: “The pandemic is still raging. We are in the second-largest surge of the pandemic, according to COVID wastewater data.
Models from Mike Hoerger suggest 2 million people a day will be infected at the peak, and 100 million or 1 in 3 people will likely get COVID overall during the entire wave.”
It is not just the height of the peak that is important. The total number of days of this wave relates to the total number of cases of JN.1.

Michael Hoerger modeling: http://pmc19.com/data/
https://twitter.com/michael_hoerger/status/1743154055415799992

1/5/24 Eric Topol MD: State-of-the-Pandemic https://buff.ly/3vsBS1y
“There isn’t adequate acknowledgement of the risk of Long Covid—or the protection from vaccination. When you think of up to 2 million Americans getting infected in a day, even if only 1% go on to suffer from chronic Covid, which can be profoundly debilitating, that’s 20,000 eventual new long haulers added to the millions here already affected. In one day. The current wave has gone on for weeks and estimates are that 4-5% of Americans have Covid now and up to 1 in 3 will have been infected during the wave cumulatively.
A recent meta-analysis of 24 studies looking at whether Covid vaccines protect from Long Covid provides encouraging evidence that there’s about 70% reduction of risk. That’s second only to not getting Covid, which of course provides 100% protection from Long Covid.”

1/4/23 OpEd by Eric Topol MD in the LA Times: The U.S. is facing the biggest COVID wave since Omicron. Why are we still playing make-believe? https://buff.ly/4aGL6Y6
"Now in its fifth year, SARS-CoV-2 has once again proved to be highly resilient, capable of reinventing itself to infect us [JN.1]. Yet we continue to make-believe that the pandemic is over, that infections have been transformed to common cold status by prior exposure(s), and that life has returned to normal. Sadly, none of this is true.”
We need to use precautions now (masks, air filtration, etc) and we need to make variant proof mucosal vaccines.
1/4/23 Erin Prater in Fortune magazine:
Why hasn't the WHO assigned a Greek letter to JN.1 "Pirola"? How it decides when to name COVID-19 variants https://buff.ly/48BSguE

Hospitals are filling:
12/31/23 Yale, Dr. Kaminski

1/3/24 Euronews: Italian hospitals collapse: Over 1,000 patients waiting to be admitted in Rome https://buff.ly/3vqosDe
Hospitals in Italy are overwhelmed with sick patients with influenza and with COVID.
Valeriani and Droghei complained of "blocked ambulances, postponed operations, clogged emergency rooms and beds blocked by COVID patients, all because of a vaccination campaign that started late".

Pediatrics
https://twitter.com/Globalbiosec/status/1741897497809997888
12/20/23 Journal of Pediatrics: High Cardiac Troponin Levels in Infants with Acute SARS-CoV-2 Infection: A Prospective Comparative study https://buff.ly/3RH73h0
152 infants hospitalized for COVID-19, 79 children with acute infections other than SARS-CoV-2, and 71 healthy controls.
High sensitivity troponin (hs-cTn) levels
"Infants with acute SARS-CoV-2 infection may show a subclinical and transient alteration of myocardial injury markers, especially in the first months of life. hs-cTn levels normalized during follow-up and were not associated with cardiac functional impairment; nevertheless, long-term consequences are unknown and should be carefully followed."
@VipinTurkur
A recent study has shown elevated troponin levels in about 1 in 3 infants infected w/ SARS-CoV-2.
Elevations were revealed to be more common in that group than in infants w/ other infections.
The risk was particularly high in the youngest infants.
7/21/23 Pediatrics: A Systematic Review of Persistent Clinical Features After SARS-CoV-2 in the Pediatric Population https://buff.ly/3S5OYdU
Review of 31 studies
Persistent clinical features beyond 3 months among children and adolescents with proven COVID-19 are common (16% or 1 in 6 children) and the symptom spectrum is wide.
Study: 1 in 6 kids have persistent COVID symptoms for 3 months after infection
1 in 6 children and teens do not fully recover from COVID infection.
12/31/23 A letter for schools from Mike Hoerger presenting data on the need for better ventilation and other mitigations in schools.
Vaccines
1/3/24 Scientific American: Vaccination Dramatically Lowers Long Covid Risk https://buff.ly/3RMFiDx or without the paywall https://archive.is/uhwDB
Receiving multiple doses of COVID vaccine before your first COVID infection greatly reduces the risk of Long COVID.
Early in the pandemic, the prevalence of Long COVID was >20%.
Now, the prevalence of Long COVID:
11% for unvaccinated people
5% for those who have had two or more doses of a COVID vaccine.
“Booster [vaccines] enhance antibodies—increasing both their numbers and their ability to bind to the virus—as well as T and B immune cells that help fight the virus.”
Studies mentioned in the Sci Am article above:
10/2023 The effectiveness of COVID-19 vaccine in the prevention of post-COVID conditions: a systematic literature review and meta-analysis of the latest research https://buff.ly/46TLboq
Meta-analysis of 24 studies found that people who received 3 doses of the COVID vaccine were 69% less likely to develop Long COVID compared to unvaccinated people.
11/22/23 BMJ: Covid-19 vaccine effectiveness against post-covid-19 condition among 589 722 individuals in Sweden: population based cohort study https://buff.ly/47vI1rD
Vaccination protection against Long COVID was dose dependent —1 dose 21%, 2 doses 59%, 3 doses 73%.
Strong association between covid-19 vaccination before infection and reduced risk of receiving a diagnosis of PCC (Long COVID).
7/1/22 JAMA: BNT162b2 (Pfizer mRNA COVID) Vaccination and Long COVID After Infections Not Requiring Hospitalization in Health Care Workers https://buff.ly/48DoTZ5
The prevalence of Long COVID in health care workers:
42% in unvaccinated
30% in those with a single dose COVID vaccine
17% with two doses
16% with three doses.
12/1/23 Scientific American: Long COVID Rates Appear to Be Decreasing https://buff.ly/3TML7Ua
1/3/24 Science Translational Medicine: Adjuvanted SARS-CoV-2 spike protein vaccination elicits long-lived plasma cells in nonhuman primates https://buff.ly/3S5MMmu
Studies in monkeys show that generating long-lived plasma cells via an adjuvanted spike protein vaccine could allow for COVID vaccines to have longer protection.
1/4/23 USA Today: Florida Surgeon General Dr. Ladapo wants to halt COVID mRNA vaccines, going against FDA https://buff.ly/3tGdNne
"The FDA stands firmly behind the safety, effectiveness and manufacturing quality of the approved and authorized COVID-19 vaccines, and respectfully disagrees with the Florida Surgeon General’s opinion," the FDA said in a statement.
"with over a billion doses of the mRNA vaccines administered, no safety concerns related to residual DNA have been identified." said the FDA.
“Ladapo has joined DeSantis on the presidential campaign trail and held various events with the governor in which scientists and medical professionals with contrarian COVID-19 views have criticized federal health authorities' management of the pandemic.”
1/5/24 Katelyn Jetelina et al: DNA in Covid-19 vaccines: 7 pieces of context missed from Florida Surgeon General’s unnecessary warning https://buff.ly/48e4R7H?
Why Dr. Ladapo is wrong about COVID mRNA vaccines.
Article from last week’s newsletter:
12/28/23 MedRxiV: BNT162b2 XBB1.5-adapted Vaccine and COVID-19 Hospital Admissions and Ambulatory Visits in US Adults https://buff.ly/47dCcyd
Article co-authored by Kaiser Permanente Southern California and Pfizer
4232 COVID cases and 19,775 controls at Kaiser Permanente in Southern California
Those who received the XBB.1.5 updated Pfizer vaccine had:
63% reduction of hospitalization
58% reduction of Emergency department visits
58% reduction of outpatient visits for COVID infection
Conclusions:
(1) XBB1.5-adapted vaccines provided significant additional protection against a range of COVID-19 outcomes and
(2) older versions of COVID-19 vaccines offered little, if any, additional protection, including against hospital admission, regardless of the number or type of prior doses received.
Interesting commentary by Michael Mina on why this article is misleading:
https://twitter.com/michaelmina_lab/status/1742397858282701104
This paper from Kaiser on the new XBB1.5 vax formulation is misleading.
NO, it does NOT say that prior vaccination w non updated XBB1.5 vaccines offer no protection.
No, it doesn’t even say the XBB1.5 updates to the vaccine formulation are important.
Here are the key conclusions.
They are WAY misleading
The major issue is w the timing [of the last vaccine dose]
The comparison is
A) a VERY recent XBB1.5 vaccine given in last 30 days,
Vs…
B) A vaccine received ~1 year or more ago!
Any effect is first and foremost owing to recency of vax
Antiviral treatments
Test2Treat.org allows any adult age 18+ to sign up in advance, or if they have a COVID infection or Flu, to get free antiviral medication whether or not you have health insurance.
If you sign up in advance of an infection, they will also send you free COVID tests.
“Please note, this program is free, and we will never request your specific payment or insurance information, nor will bill or contact any insurance provider you may have.”
12/31/23 FT: Expired Pfizer Covid antiviral drugs set to cost Europe $2.2 Billion, data shows https://buff.ly/3NPG9Cu
The UK, France, Spain and Italy could have made Paxlovid more accessible without using up their supplies. More than 1.5 Million doses of Paxlovid worth $1.1 Billion have expired already and by the end of February 2024, a total of 3.1 Million courses of Paxlovid will have expired, costing European health systems $2.2 Billion.
Long COVID
1/4/24 Nature (Wust lab): Muscle abnormalities worsen after post-exertional malaise in Long COVID https://buff.ly/3vp9GN0
Post-exertional malaise (PEM) in Long COVID patients was seen the day after they first exercised. Controls had some post-exertional fatigue as well.
In Long COVID, skeletal muscle structure is associated with a lower exercise capacity and local and systemic metabolic disturbances. Peripheral.
Severe exercise-induced muscle damage and tissue infiltration of amyloid deposits in skeletal muscles of patients with Long COVID worsened after post-exertional malaise was triggered.
Skeletal muscles in Long COVID:
More highly fatigable glycolytic skeletal muscle fibers
Lower fatigue-resistant type I muscle fibers in females only.
The lower exercise capacity in long COVID patients is associated with a greater proportion of high-fatigable glycolytic fibers and lower mitochondrial function (a fiber-type shift towards a less oxidative, more glycolytic phenotype).
The pathophysiology of post-exertional malaise (PEM) includes:
an acute exercise-induced reduction in skeletal muscle mitochondrial enzyme activity (lower mitochondrial respiration)
Blood and skeletal muscle metabolomes in Long COVID patients show higher glycolytic metabolites and lower TCA cycle metabolites.
an increased accumulation of amyloid-containing deposits in skeletal muscle, next to capillaries and in the extracellular matrix between muscle fibers.
signs of severe exercise-induced muscle damage (necrosis) and subsequent regeneration
a muscle fiber-type shift towards a less oxidative, more glycolytic phenotype.
a blunted exercise-induced T-cell response in skeletal muscle.
higher skeletal muscle infiltration of CD68+ macrophages and CD3+ T-cells suggests a locally disturbed immune response in patients with long COVID.
Results confirm previous suggestions of impaired peripheral oxygen extraction in skeletal muscles in long COVID patients and a higher concentration of amyloid deposits in skeletal muscle, but there was no evidence of blocked capillaries within the skeletal muscle.
“In conclusion, this study reveals that local and systemic metabolic disturbances, severe exercise-induced myopathy, infiltration of amyloid-containing deposits, and immune cells in skeletal muscles of long COVID are key characteristics of post-exertional malaise. While these explain the symptomatology of post-exertional malaise in long COVID, the molecular pathways underlying these alterations in patients suffering from post-exertional malaise remain to be determined.”
Fig. 1: Lower exercise capacity in patients with long COVID.
Fig. 2: Skeletal muscle alterations (glycolytic fibers) are associated with exercise capacity in patients with long COVID.
Fig. 3: Metabolic and mitochondrial dysfunction in long COVID patients worsens with post-exertional malaise.
OXPHOS, SDH enzyme
Muscle and blood metabolomes show higher glycolytic metabolites and lower TCA cycle metabolites.
Fig. 4: More amyloid-containing deposits in skeletal muscle, but not located inside capillaries or lymphatic vessels.
Fig. 5: Pathological features in skeletal muscle in patients with long COVID.
In LC, more atrophy, necrosis, internal nuclei (fiber repair), regeneration, CD3+ Tcell infiltration, higher CD68+ Macrophages.
Large areas of necrotic fibers were observed in 36% of patients with long COVID after exhaustive exercise


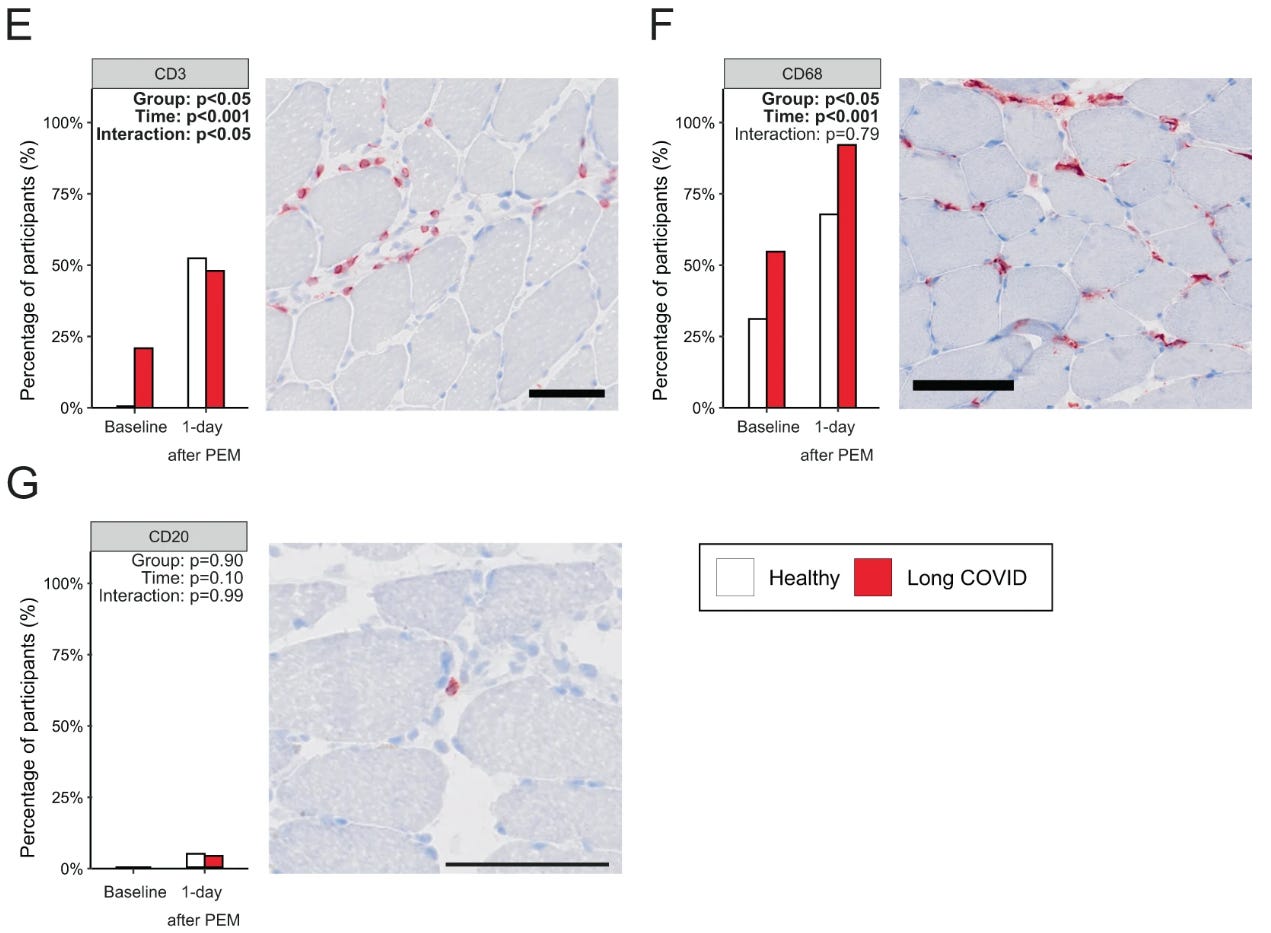
Fig. 6: Similar concentrations of nucleocapsid protein in skeletal muscle in patients with long COVID as control.

1/4/23 Tweet thread from Rob Wust on his lab’s new paper in Nature:
https://twitter.com/RobWust/status/1742856116181028994
Summary:
There are skeletal muscle changes in Long COVID (LC) patients that worsen after exercise.
Muscle pain, fatigue and weakness and PEM is seen in LC patients after exercise.
In some LC patients, exercise caused extensive muscle damage (myopathy and muscle necrosis even).
Skeletal muscle mitochondrial function and metabolism were abnormal in patients with LC and this worsened when post-exertional malaise (PEM) was triggered with exercise.
Intense exercise is not good for patients with long COVID!
Amyloid:
Amyloid deposits were found between skeletal muscle fibers and not in capillaries or endothelial cells, as had been expected.
There were higher amounts of amyloid in the skeletal muscle of people with LC than in controls.
Amyloid deposits increased in the muscles of LC patients after exercise.
SARS-2 viral particles were not found inside muscle cells.
This paper took months to be reviewed/edited. In the meantime, the Wust lab and colleagues have continued to work on understanding how to reduce PEM in Long COVID. “Stay tuned!”

What is amyloid?
Amyloid Protein - an overview | ScienceDirect Topics https://buff.ly/3vrhU7n
Caleb E. Finch, in The Biology of Human Longevity, 2007
1.3.4 Amyloids and Inflammation
Changlin Liu, Yong Zhang, in Advances in Protein Chemistry and Structural Biology, 2011
Amyloid proteins, mainly including amyloid-β peptides, prion proteins, α-synuclein, copper/zinc superoxide dismutase, as well as the bacterial protein RepA, are characterized by the deposition in a variety of tissues or cells as aggregated species (amyloids or insoluble deposits or inclusions) that share a distinctive β-sheet-rich fibrillar ultrastructure.
Although the amyloid is predominantly proteinaceous, careful examination of disease tissues and cells has revealed the presence of a significant quantity of polyanionic species including nucleic acids and polysaccharides associated with the amyloid. For example, in the brain tissues from victims of Alzheimer's disease, nucleic acids have been detected in neurofibrillary tangles and intracellular inclusions primarily composed of the tau protein, as well as in senile plaques composed of the amyloid-β peptides.
5/2023 Lancet neurology: Biomarker called α-synuclein can tell if someone has Parkinson’s disease. Alpha-synuclein can pick up if a person has very early disease and it may be a target for therapy for Parkinson’s disease in the future.
—----
1/2024 American Journal of Emergency Medicine: Remission of severe forms of long COVID following monoclonal antibody (MCA) infusions: A report of signal index cases and call for targeted research https://buff.ly/3H8EcgH
Three cases of complete remission of severe Long COVID within 1 week of monoclonal antibody infusion.
Reviewed previously when this was a pre-print.
1/4/24 Regarding ME/CFS studies that were not followed up upon until Long COVID happened


1/3/24 Nature: Long COVID is a double curse in low-income nations — here’s why https://buff.ly/3THR70C
“Not only is the prevalence of the condition poorly understood, but it’s also often ignored by physicians and the wider public.”

1/2/24 Nature Reviews Cardiology: Cardiovascular autonomic dysfunction in post-COVID-19 syndrome (Long COVID): a major health-care burden https://buff.ly/47plBYm
Authors from Sweden, Austria, Canada, United States, UK
Cardiovascular autonomic dysfunction (CVAD) is a malfunction of the cardiovascular system caused by deranged autonomic control of circulatory homeostasis.
"In this Review, we define CVAD and its major forms that are encountered in post-COVID-19 syndrome, describe possible CVAD aetiologies, and discuss how CVAD, as a component of post-COVID-19 syndrome, can be diagnosed and managed. Moreover, we outline directions for future research to discover more efficient ways to cope with this prevalent and long-lasting condition."
“Key points
Cardiovascular autonomic dysfunction (CVAD), in particular postural orthostatic tachycardia syndrome (POTS) and inappropriate sinus tachycardia, are among the most frequent and distinct phenotypes of post-COVID-19 syndrome; one-third of highly symptomatic patients can be affected.
CVAD arises from a malfunction of the autonomic control of the circulation, and can involve failure or inadequate or excessive activation of the sympathetic and parasympathetic components of the autonomic nervous system.
As well as global circulatory disturbances, CVAD in post-COVID-19 syndrome can manifest as microvascular and endothelial dysfunction, with local symptoms such as headache, brain fog, chest pain, dyspnoea and peripheral circulatory symptoms, including skin discolouration, oedema, Raynaud-like phenomena, and heat and cold intolerance.
A structured diagnostic work-up based on a detailed patient history, cardiovascular autonomic testing, long-term electrocardiogram and blood-pressure monitoring, and ancillary cardiac and peripheral vascular tests will lead to an appropriate diagnosis.
Management of CVAD in post-COVID-19 syndrome should involve a correct diagnosis, patient education, and both non-pharmacological and pharmacological methods; a tailored exercise training programme, blood volume expansion and compression garments are especially effective.
Pharmacological approaches target heart rate control, blood volume expansion, promotion of vasoconstriction and venoconstriction, and reduction of hyperadrenergic drive.”

12/31/23 Washington Post: Four years on, Long covid still confounds us. Here’s what we now know. https://buff.ly/41Lwoec
In 2022, 7% of Americans (18 million people) reported that they have had Long COVID symptoms and half improved.
Limitations on ability to work and strain on the healthcare system.
"Believe your patient!", David Putrino
Other news:
1/4/24 CNN: These twins don’t share a birthday, or a birth year https://buff.ly/3NSg7yz
Baby Ezra was born on Dec 31, 2023 at 11:48pm.
Baby Ezekiel arrived on Jan 1, 2024 at 00:28 am.

12/22/23 Double the uterus, double the babies, double the birthdays: Alabama mom delivers rare twins at UAB https://buff.ly/47mgE2y
Dicavitary twins- Baby A, named Roxi, was delivered vaginally on December 19th and Baby B, named Rebel, was delivered 10 hours later by c-section on December 20th.


12/12/23 JAMA: Cannabis Exposure and Adverse Pregnancy Outcomes Related to Placental Function https://buff.ly/3RJ0p9T
"Maternal cannabis use was associated with adverse pregnancy outcomes, including small for gestational age, preterm birth, stillbirth and hypertensive disorders of pregnancy, linked to placental function, researchers reported.”
AI:
1/3/24 Science: TBscreen: A passive cough classifier for tuberculosis screening with a controlled dataset https://buff.ly/41PeXt6
Smartphone app listens to passive cough in Nairobi and using deep learning AI, it can tell if someone has Tuberculosis or not, and can estimate associated bacterial burden and disease severity.
1/2/24 JAMA: Diagnostic Accuracy of a Large Language Model in Pediatric Case Studies https://buff.ly/4aHEZ5N
ChatGPT version 3.5 reached an incorrect diagnosis in 83 out of 100 pediatric case challenges. Among the incorrect diagnoses, 72 were actually incorrect and 11 were clinically related to the correct diagnosis but too broad to be considered correct.
Thank you so much for your invaluable newsletters! You do us a great service in keeping us informed about COVID.
Always appreciate your posts, and this one in particular. Thank you for breaking down the long COVID muscle/PEM research the way you did. I tried reading that study last night and it was hard to fully grasp.