

COVID news & more, 2/24/24

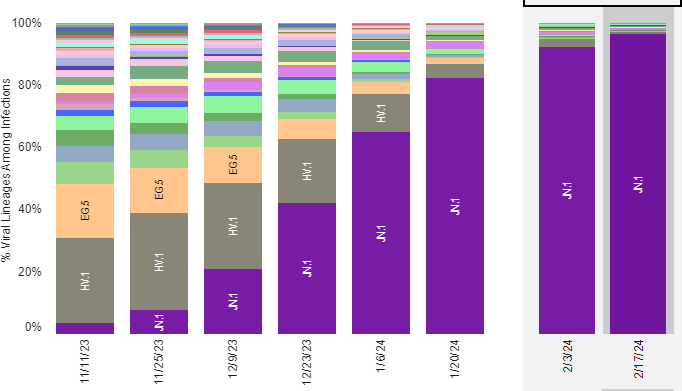
JN.1 continues to be the only variant causing COVID cases now. A new study confirmed that the XBB.1.5 vaccine is effective against JN.1. It turns out that responses to COVID vaccines are better than previously thought. Antibody formation after vaccination shows two phases: an initial rapid decrease (waning) in SARS-CoV-2 spike IgG antibodies, followed by stabilization of antibody levels for at least 7 to 9 months. This is consistent with typical B cell physiology.
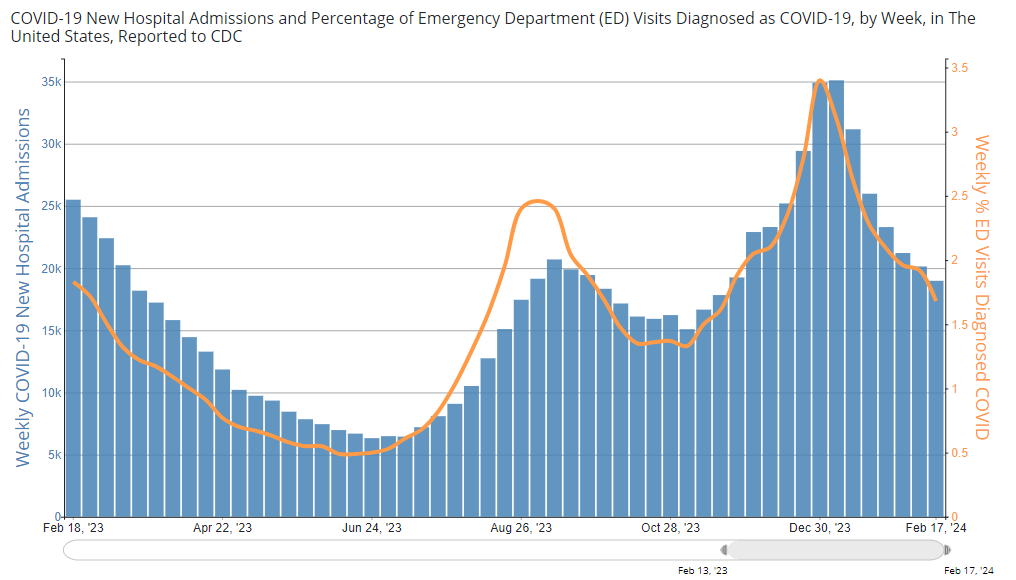
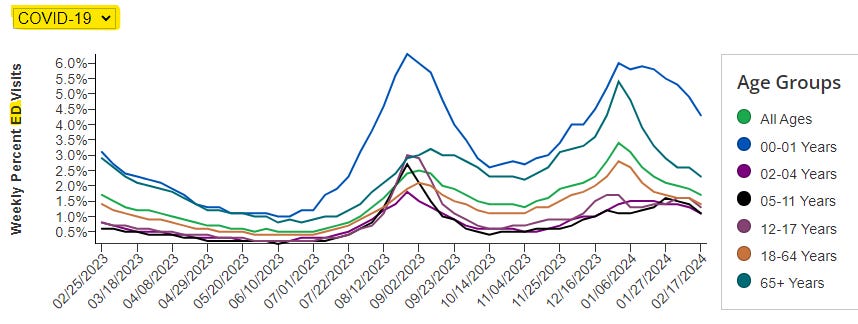
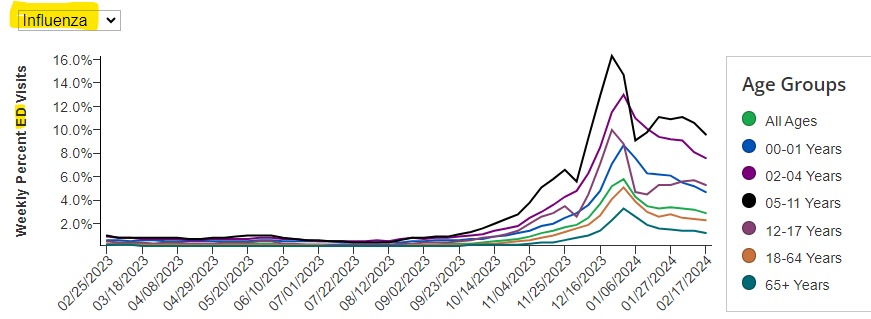
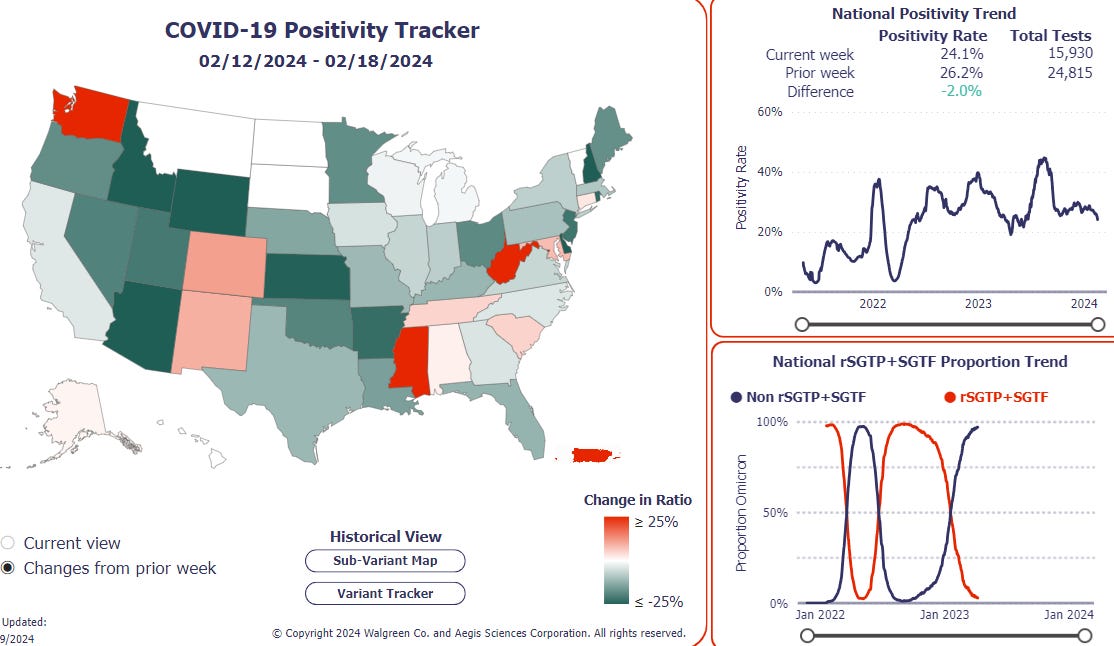
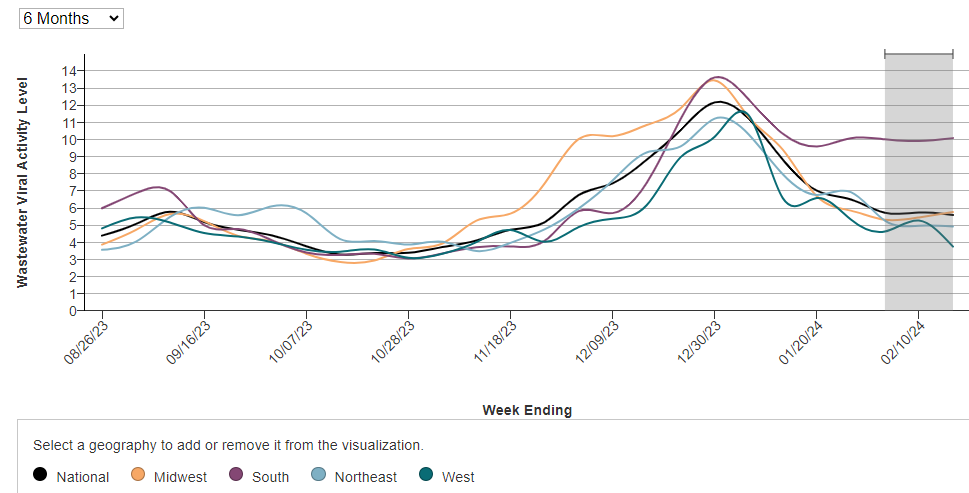
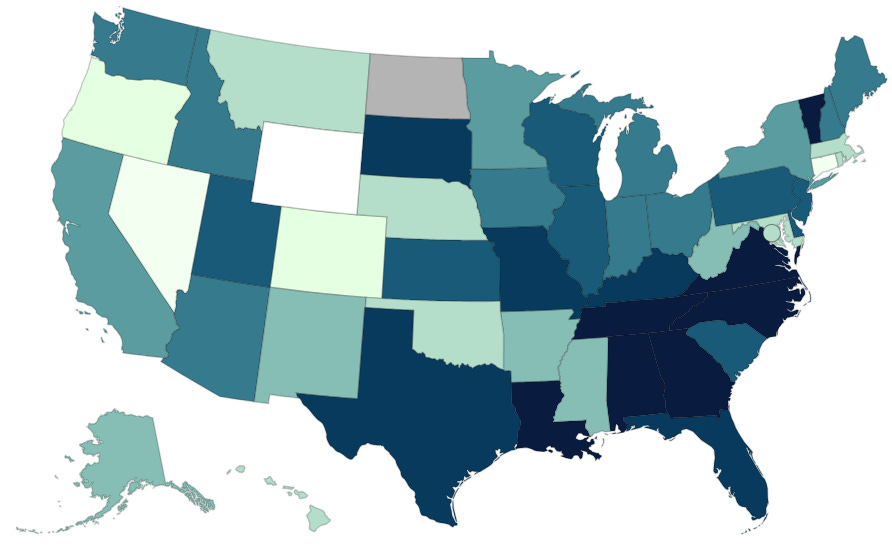
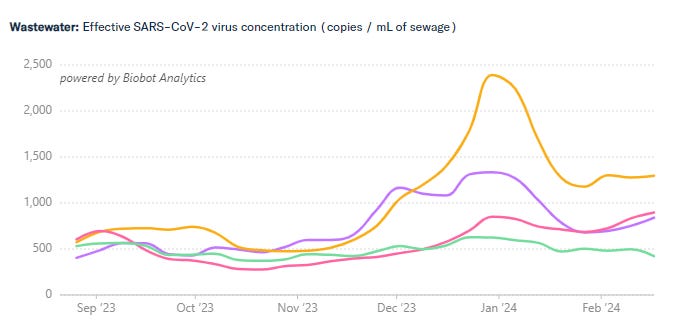
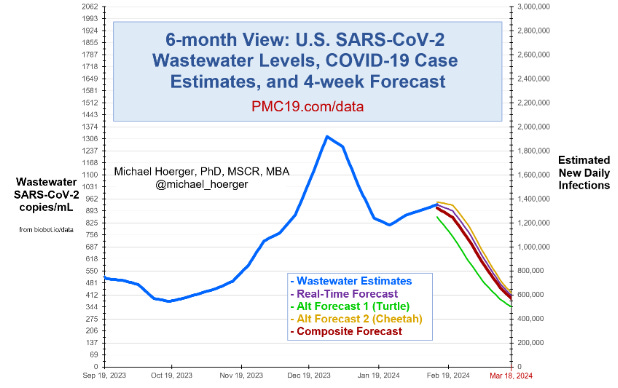
SARS-CoV-2 virus levels are still in the “HIGH” range in the United States, with an uptick of COVID infections in the southern states. Tennessee has exceptionally high levels of COVID circulating, followed by Texas, Oklahoma and Virginia. Per JP Weiland, wastewater levels of COVID are decreasing and hospitalizations for COVID are mirroring the decline of cases. There are still about 700,000 new COVID cases each day in the U.S. as seen by wastewater COVID levels and about 18,000 people hospitalized with COVID now. Emergency department visits for COVID are decreasing across all age groups, as are ED visits for influenza. A descendant variant of JN.1 called JN.1.23 has been found in a few countries including Brazil, but so far it is just being watched.
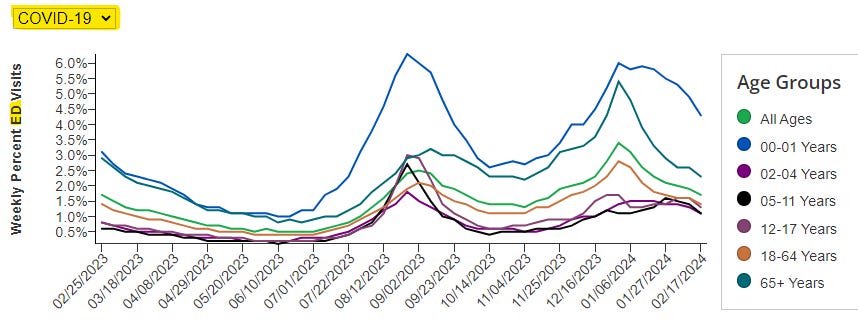
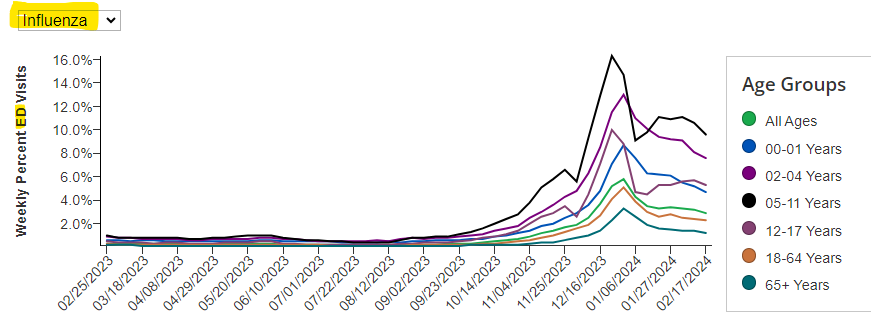
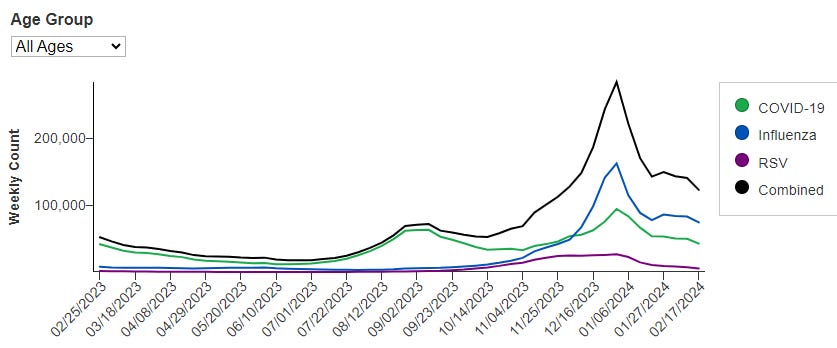
From: CDC: Weekly ED visits for respiratory illnesses, by age and disease
Acute COVID infections, General COVID info
A study from Egypt looked for SARS-CoV-2 virus in routine colonoscopy and upper gastrointestinal endoscopy tests and found that if the patient had a prior COVID infection, 37% were positive for SARS-CoV-2 in their upper gastrointestinal tract and 17% were positive for SARS-2 in their colon and lower gastrointestinal tract. The authors concluded “Gut mucosal tissues can act as a long-term reservoir for SARS-CoV-2, retaining viral particles for months following the primary COVID-19 infection. Smokers and individuals with diabetes may be at an increased risk of persistent viral gut infection.”
Looking at the brains of people who had neurologic symptoms before they died of acute COVID infections, researchers from Charite in Berlin found that even without direct infection of the brain by SARS-CoV-2, the vagus nerve senses COVID infection in the body’s organs (lungs, heart, intestine) and sends an inflammatory message to the brainstem causing neurologic symptoms in acute COVID infections. It makes sense that this could be happening during Long COVID as well, if there is viral persistence somewhere in the body, although this particular study did not look at that.
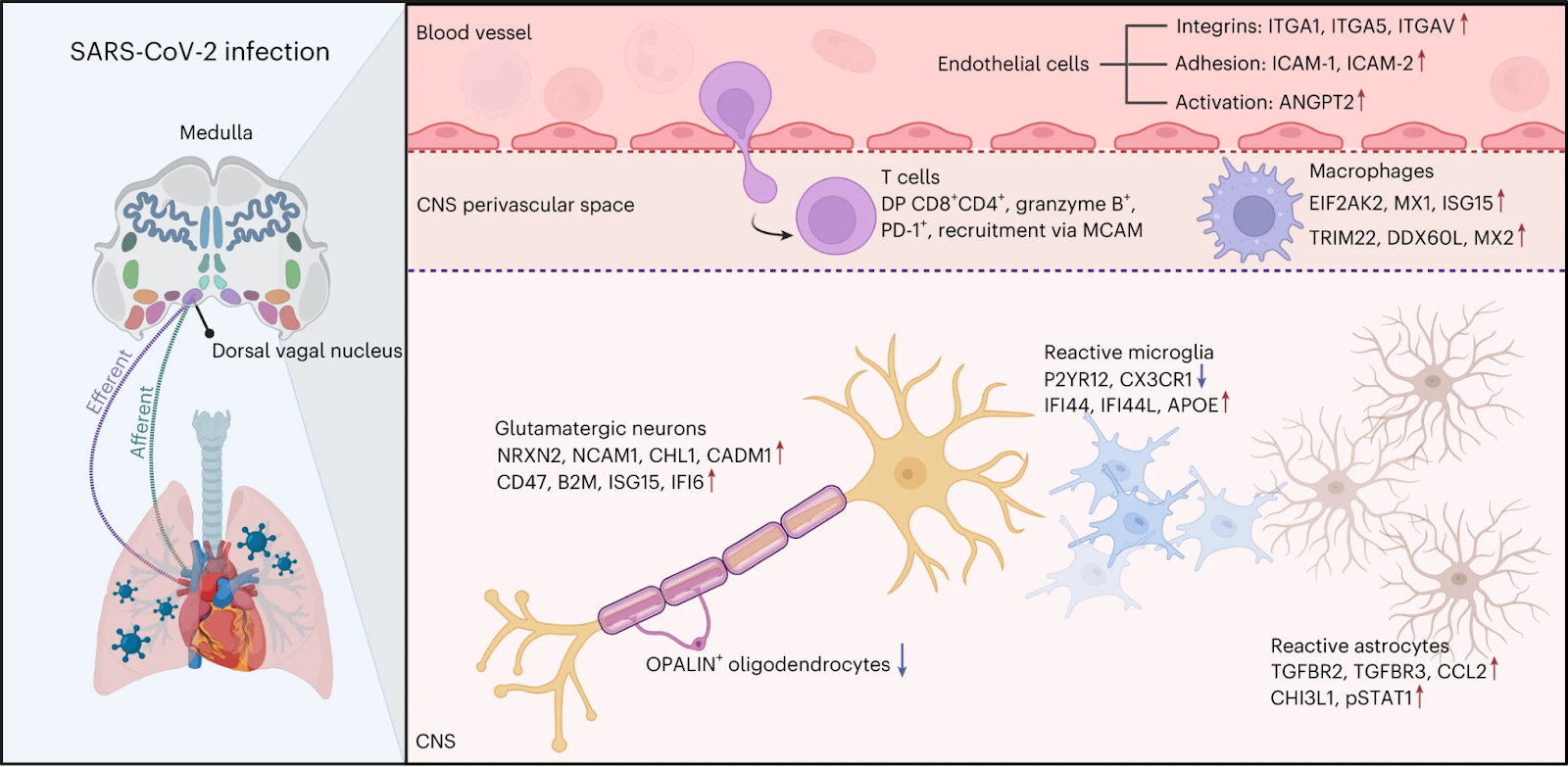
Figure 5: Multiomic analysis of the medulla oblongata from patients that died of COVID-19, showing strong activation of endothelial cells, increased permeability of the BBB and altered T cell and microglial activation, but also implications of connections between periphery (for example, heart) and brain.
The Washington Post reported that four “nonprofits” that spread medical misinformation about vaccines and COVID treatments collectively received more than $118 million in contributions and grants between 2020 and 2022, “enabling the organizations to deepen their influence in statehouses, courtrooms and communities across the country.” Over half of donations were made via “donor-advised funds” which allow individuals to obscure their identities.
Long COVID
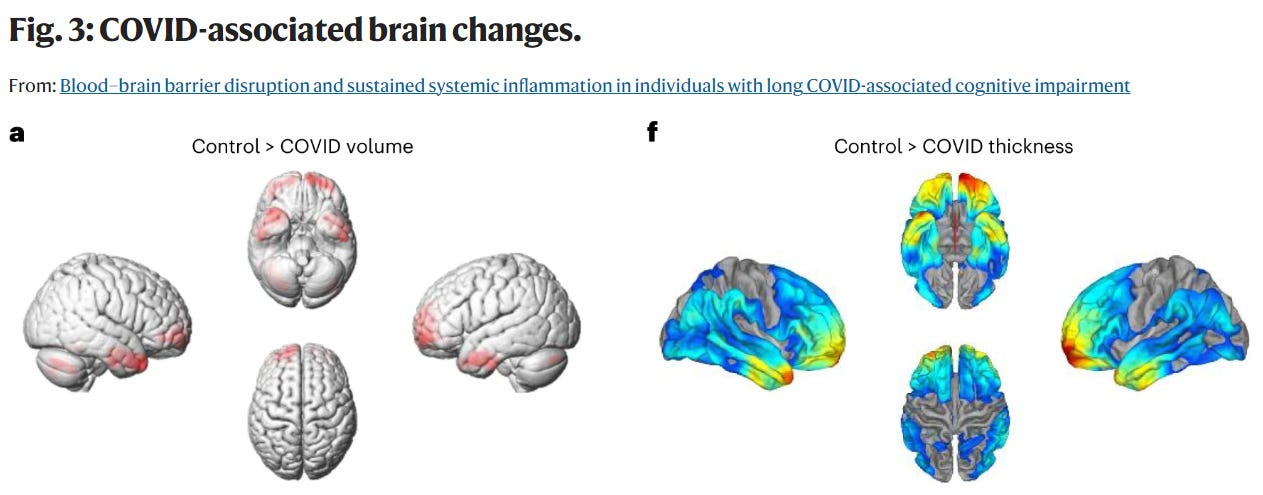
The blood brain barrier (BBB) usually protects the brain from toxins that could be circulating in the bloodstream. This week, a group from Trinity College in Ireland showed that a disruption of the BBB in Long COVID causes blood vessels in the brain to become leaky. Inflammatory substances from the body are then able to cross into the brain leading to Long COVID ‘brain fog’ and cognitive problems including memory loss and difficulty thinking. The researchers used dynamic contrast-enhanced MRI (DCE-MRI) to show which areas of the brain had the “leaky” BBB. They also found that people with Long COVID brain fog had structural brain changes including a reduction in brain volume. In addition, they found dysregulation of the coagulation system pathways in people with Long COVID and brain fog.
Fig. 2: BBB disruption in long COVID-associated brain fog.
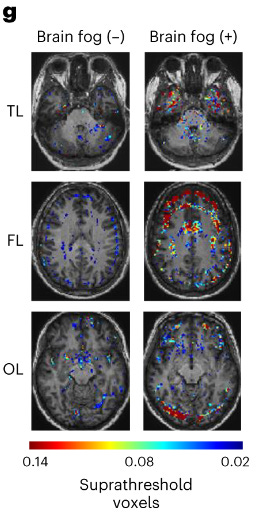
Figure 2g) Leaky BBB as seen by BBB permeability maps on Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) at the level of the temporal lobes (TL), frontal lobes (FL) and occipital lobes (OLs) showing enhanced BBB permeability in cases of Long COVID with brain fog.
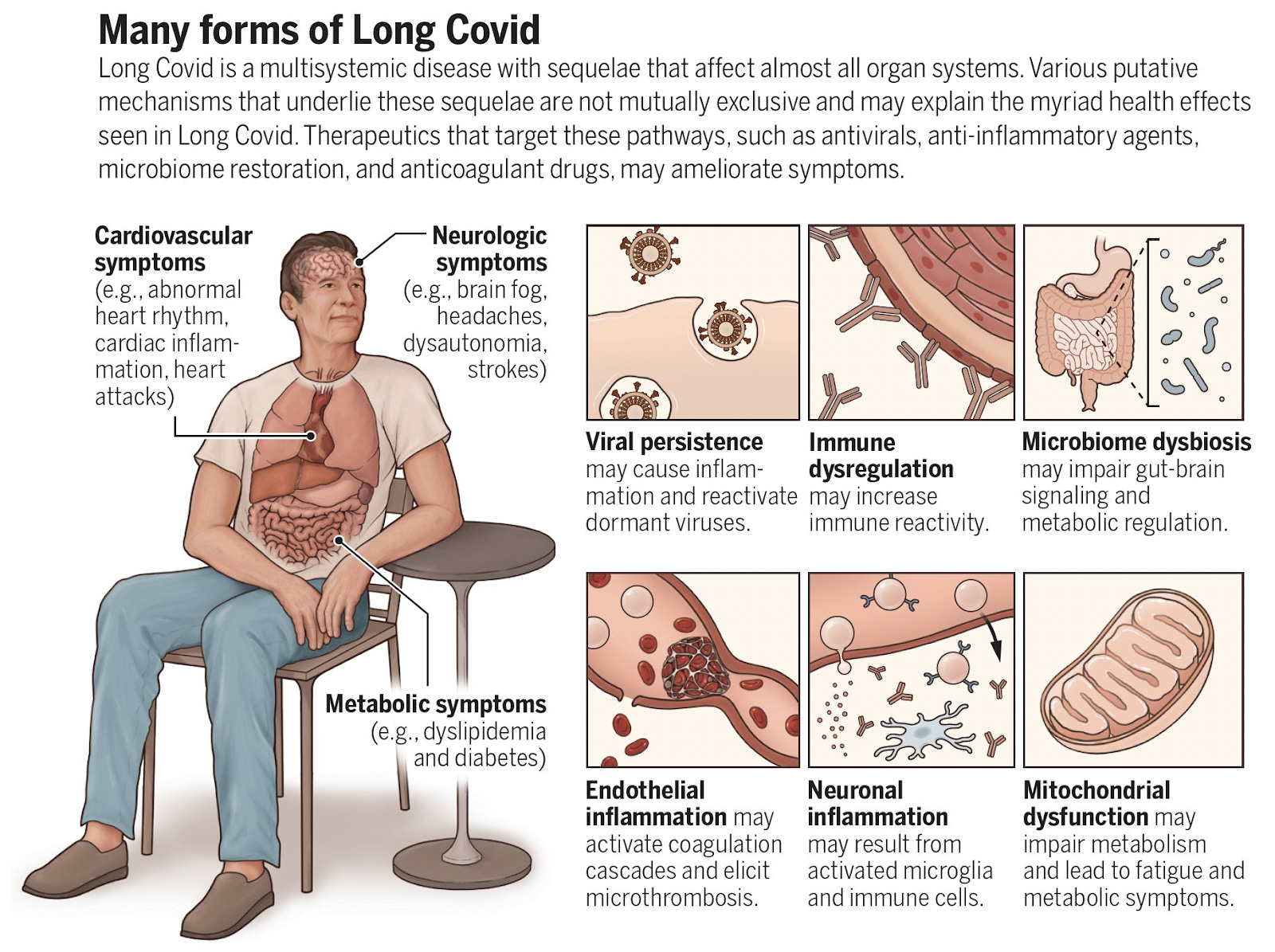
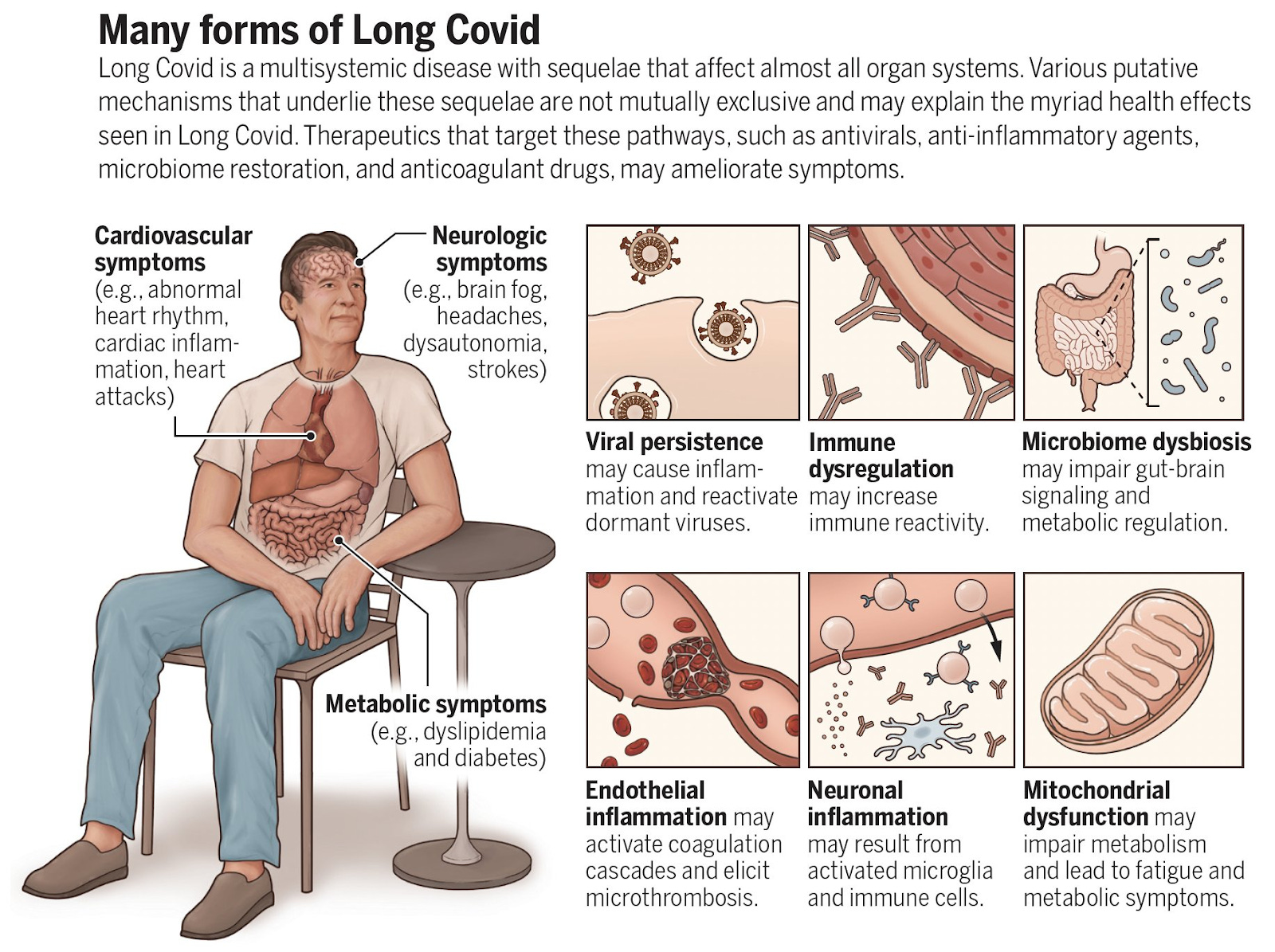
Ziyad Al-Aly and Eric Topol wrote a paper in Science magazine entitled “Solving the puzzle of Long Covid” in which they reviewed what we now know about Long COVID including possible causes and the different subtypes of Long COVID. Prevention of Long COVID using vaccines and Paxlovid, Ensitrelvir and Metformin were also discussed, as well as the use of physical mitigations like better indoor air quality and masking. In addition, they looked at how acute COVID reinfections increase the risk of getting Long COVID and how we need to focus on finding treatments for Long COVID now. The authors also wrote a blog post called “Towards Solving the Long Covid Puzzle” in which they discussed this week’s Long COVID findings.
From: “Solving the puzzle of Long Covid”
The PolyBio Research Foundation announced grants to scientists in its LongCovid Research Consortium (LCRC). According to the PolyBio website, over a dozen institutions globally participate in the LCRC, including Harvard Medical School, University of Pennsylvania, the Icahn School of Medicine at Mount Sinai, Yale School of Medicine, University of California San Francisco (UCSF), the J. Craig Venter Institute, the French National Institute for Health & Medical Research/ESPOIRS and the Karolinska Institutet among others. According to a tweet from PolyBio, most studies funded will be looking at SARS-CoV-2 viral persistence and the impact of viral activity on Alzheimer’s and cardiovascular diseases. A list of all topics to be studied is in my COVID notes below.
A study from Cambridge shows that persistently elevated interferon-gamma (IFN-γ) from peripheral blood mononuclear cells (PBMCs) after COVID infection may be a biomarker for Long COVID. Resolution of Long COVID symptoms was associated with IFN-γ decreasing to baseline levels.
Immunocompromised individuals can get persistent COVID infections that can allow the SARS-CoV-2 virus to continue to mutate in their bodies. It turns out that 0.1–0.5% of COVID infections in healthy people become persistent as well with rebounding high viral loads that can last for at least 60 days. High viral loads suggest actively replicating virus and some new viral mutations were noted over time. People with persistent SARS-CoV-2 infections had more than 50% higher odds of reporting Long COVID than people without long term, persistent infections.
A new small study in Nature magazine looked at post-infectious myalgic encephalomyelitis/chronic fatigue syndrome (PI-ME/CFS). They found that fatigue in PI-ME/CFS is related to decreased activity of the right temporal-parietal junction in the brain. T cell exhaustion, as seen by elevated PD-1 in cerebrospinal fluid (CSF), dysregulation of catecholamine synthesis in the hypothalamus, and autonomic dysfunction with increase in sympathetic and a decrease in parasympathetic activity was found in people with PI-ME/CFS.
In addition, there were sex differences noted in PI-ME/CFS in immune system responses related to peripheral blood mononuclear cells (PBMCs) gene expression, increased oxidative stress noted in muscles via different pathways in men versus women, and sex differences in CSF metabolites. Their findings and possible mechanisms that cause PI-ME/CFS, including Long COVID ME-CFS, are summarized in the figure below:
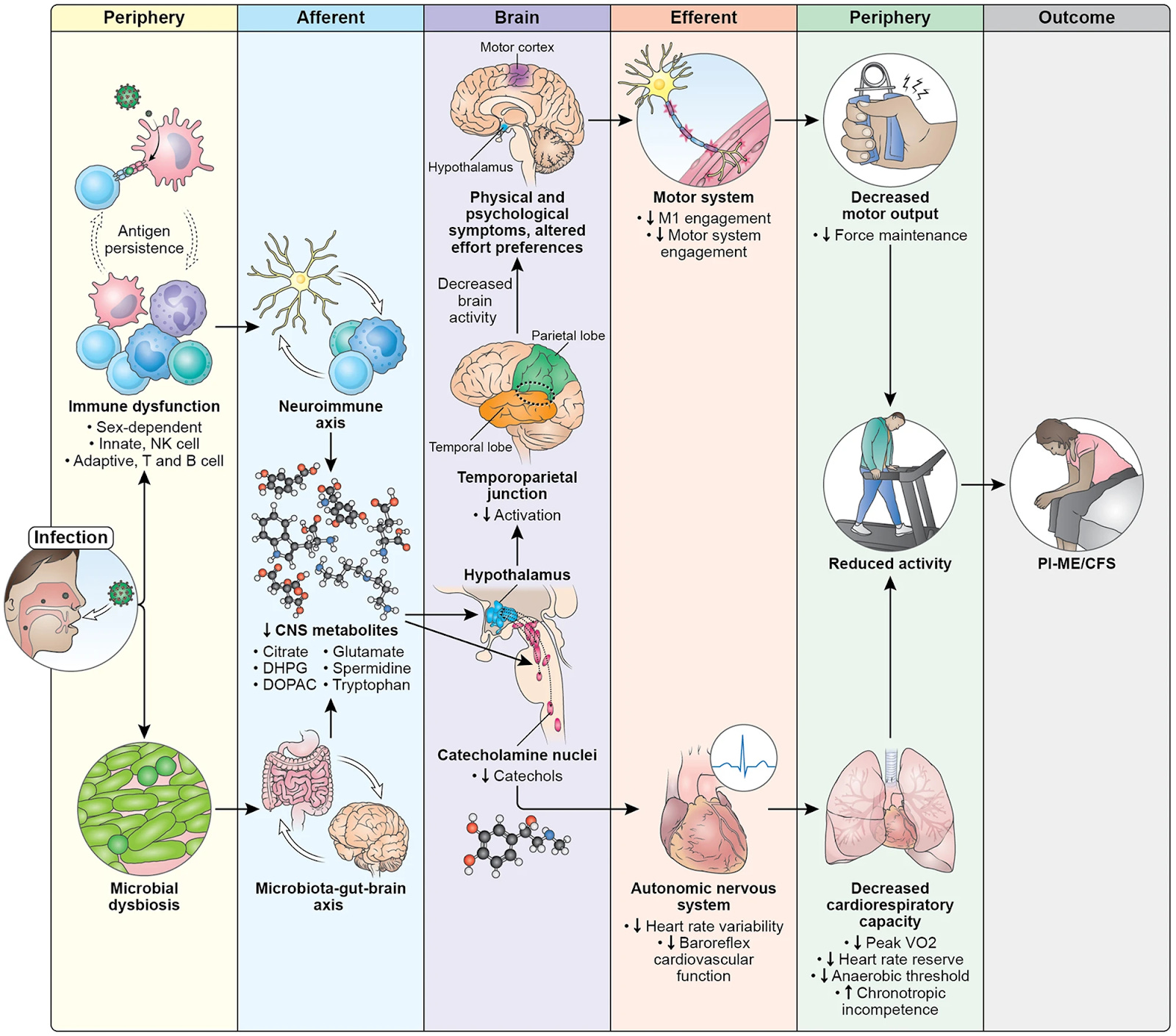
Fig. 10: Pathophysiology of PI-ME/CFS
In non-COVID news, generative AI has high environmental costs because it consumes a lot of energy to run. The Alabama Supreme Court ruled this week that embryos created through in vitro fertilization (IVF) are considered children. With this new ruling, if a frozen embryo does not thaw correctly, IVF physicians could be liable for civil charges for “destroying” an embryo. People are not allowed to transport their frozen embryos out of Alabama now either. Several clinics have stopped doing IVF in Alabama because of the new ruling.
Niacin has been used to treat high cholesterol, but a new study shows that niacin can actually increase vascular inflammation and major adverse cardiac events (MACE).
Japanese researchers have discovered a new species called the skeleton panda sea squirt. These 2 cm creatures have panda-like markings on their heads and blood vessels that look like a skeleton along their bodies.

From CNN: The skeleton panda sea squirt
Have a good rest of your weekend,
Ruth Ann Crystal MD
COVID news notes:
US Variant tracker: https://covid.cdc.gov/covid-data-tracker/#variant-proportions

Variants in locations around the globe: https://outbreak.info/
CDC COVID data tracker: https://covid.cdc.gov/covid-data-tracker/index.html#datatracker-home

CDC COVID Hospitalizations (blue) and Emergency Room (orange) visits tracker: https://covid.cdc.gov/covid-data-tracker/index.html#trends_weeklyhospitaladmissions_7dayeddiagnosed_00
Weekly ED visits for respiratory illnesses, by age and disease: https://www.cdc.gov/ncird/surveillance/respiratory-illnesses/index.html
Walgreens positivity rate: https://www.walgreens.com/businesssolutions/covid-19-index.jsp
US Wastewater Monitoring:
CDC wastewater reporting: https://www.cdc.gov/nwss/rv/COVID19-nationaltrend.html
CDC wastewater map: https://www.cdc.gov/nwss/rv/COVID19-currentlevels.html
Note the South

Biobot: https://biobot.io/data/
Biobot is not reporting as many sites as Verily from the CDC. See JP Weiland’s tweet below. He mapped out hospitalizations which do not show the same uptick or plateau in cases that Biobot does.
National SARS-CoV-2 data from Sara Anne Willette: https://iowacovid19tracker.org/
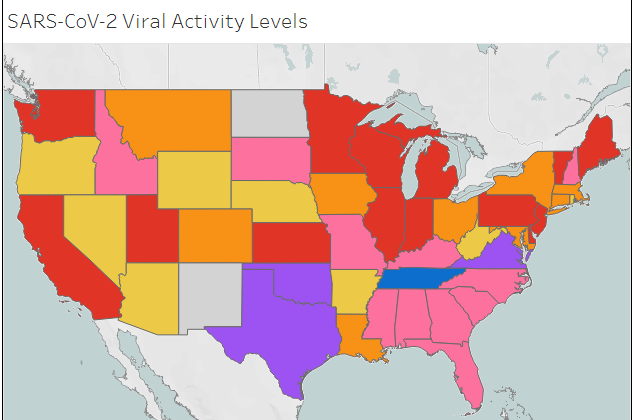
Tennessee is extremely high

Wastewater SCAN: https://data.wastewaterscan.org/
California statewide view https://buff.ly/3YObiul
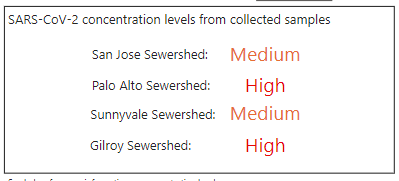
Sewer Coronavirus Alert Network (SCAN) project by Stanford University:
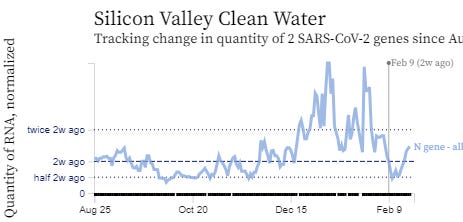
Santa Clara County wastewater: https://covid19.sccgov.org/dashboard-wastewater
CDC Respiratory vaccination trends: https://www.cdc.gov/respiratory-viruses/data-research/dashboard/vaccination-trends-adults.html
From VioletBlue’s Pandemic Round-Up: https://www.patreon.com/posts/pandemic-roundup-98981451
Per SCAN, California levels are decreasing but some very high levels.
“Sausalito, Novato, San Francisco, and Gilroy are all trending down, while Orange County (Laguna Niguel sewershed) and Palo Alto are rising again. Oakland‘s downturn doesn't look like it'll hold and is edging up; this is probably the beginning of what we'll see more of with zero covid isolation and kids in school/people forced to work sick. In Santa Clara County, which may never get a rest, San Jose and Sunnyvale are in "Medium" while Palo Alto, and Gilroy are in “High.” Marin is still in Medium while virus levels are very high and the big red arrow says it’s primed to increase. San Rafael is still a hotspot.”
JP Weiland: https://twitter.com/JPWeiland
2/22/24 https://twitter.com/JPWeiland/status/1760842109945299115

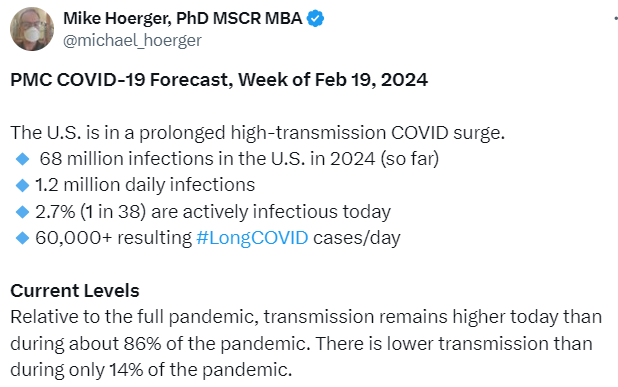
Michael Hoerger modeling: http://pmc19.com/data/
https://twitter.com/michael_hoerger/status/1760023277635023003
Variants
https://twitter.com/JPWeiland/status/1760513382472372608

Acute COVID infections, General COVID info
1/2024 Endoscopy International Open (Egypt): Incidence of persistent SARS-CoV-2 gut infection in patients with a history of COVID-19: Insights from endoscopic examination https://buff.ly/3UNyhpw
Endoscopic biopsies in patients with previous COVID-19 infection undergoing upper or lower gastrointestinal endoscopy (UGE or LGE).
No significant differences were observed between patients with positive and negative immunostaining regarding the number of previous COVID-19 infections, time since the last infection, symptoms, or vaccination status.
The incidence of positive immunostaining for SARS-CoV-2 was significantly higher in UGE biopsies than in LGE biopsies (37.34% vs. 16.87%, P=0.002).
Gut mucosal tissues can act as a long-term reservoir for SARS-CoV-2, retaining viral particles for months following the primary COVID-19 infection. Smokers and individuals with diabetes may be at an increased risk of persistent viral gut infection.
2/16/24 Nature Neuroscience (Charite Berlin): Proteomic and transcriptomic profiling of brainstem, cerebellum and olfactory tissues in early- and late-phase COVID-19 https://buff.ly/3USqgj7
single-nucleus transcriptomes and proteomes of brainstem tissue from deceased individuals at various stages of COVID-19.
2 patterns of reaction to severe systemic inflammation,
direct focus on cranial nerve nuclei nerves
diffuse pattern affecting the whole brainstem.
“bystander effect of the respiratory infection that spreads throughout the vascular unit and alters the transcriptional state of mainly oligodendrocytes, microglia and astrocytes, while alterations of the brainstem nuclei could reflect the connection of the immune system and the central nervous system via, for example, the vagus nerve.”
Our results indicate that even without persistence of SARS-CoV-2 in the central nervous system, local immune reactions are prevailing, potentially causing functional disturbances that contribute to neurological complications of COVID-19.”
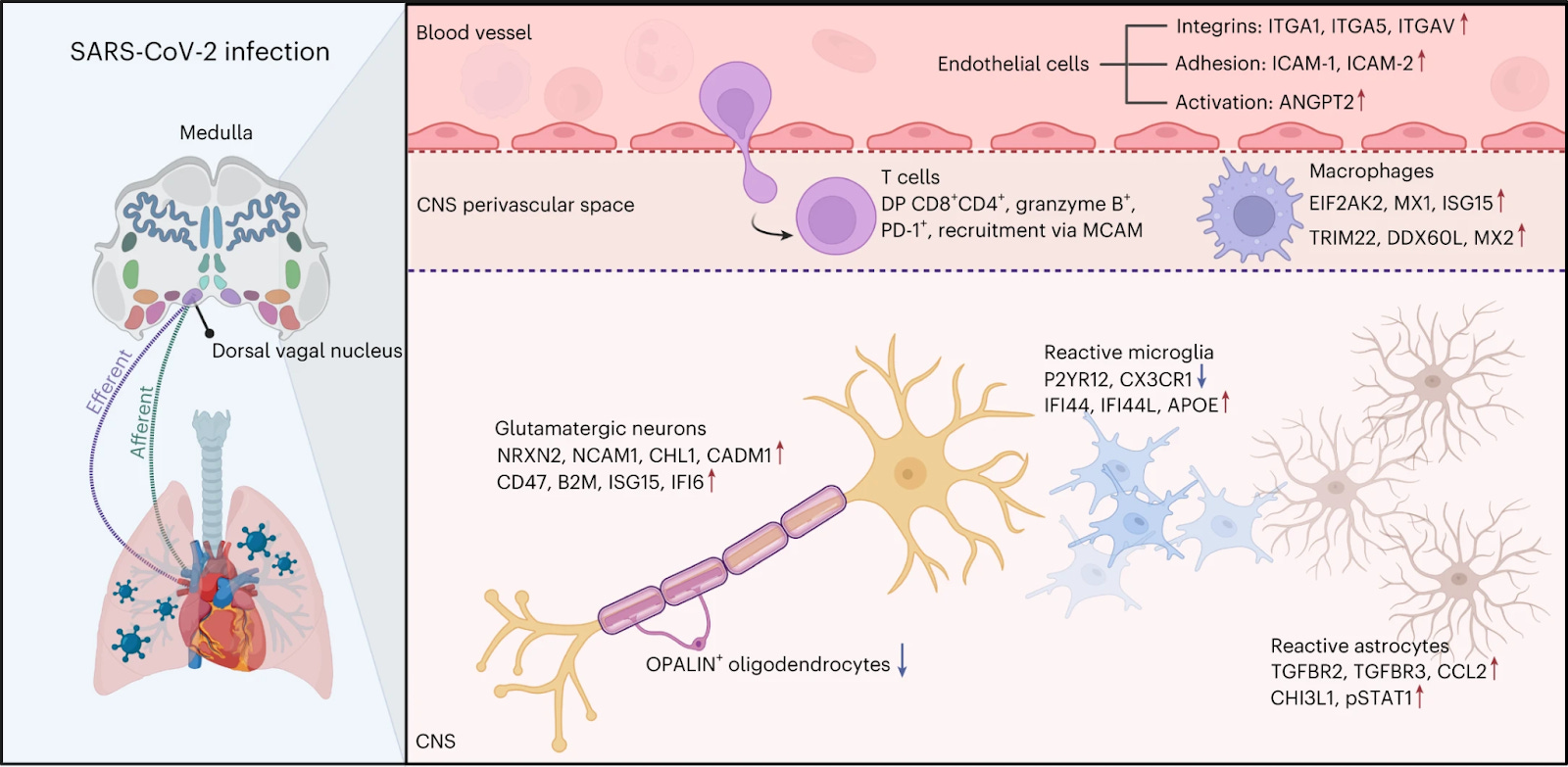
Figure 5: Multiomic analysis of the medulla oblongata from patients that died of COVID-19, showing strong activation of endothelial cells, increased permeability of the BBB and altered T cell and microglial activation, but also implications of multilayered afferent and efferent polysynaptic axonal connections between periphery (for example, heart) and brain. Important up- and downregulated genes and/or proteins are shown for certain cell types in the different CNS compartments.
2/16/24 EurekaAlert (Charite Berlin): How COVID-19 affects the brain https://buff.ly/3uxegJ5
Neurologic symptoms in COVID infection is from inflammation from the body and not from direct infection of SARS-CoV-2 in the brain.
Neurological symptoms are a side effect of the strong immune response the body deploys to defend against the virus.
No signs of direct infection of the brain. The vagus nerve senses COVID infection in the body’s organs (lungs, heart, intestine) and sends the inflammatory message to the brainstem which leads to neurologic symptoms in acute COVID infection.
Brain is reacting to inflammation in the body via the nuclei of the vagus nerve. These are nerve cells located in the brainstem that extend all the way to organs such as the lungs, intestine, and heart.
“In simplified terms, our interpretation of our data is that the vagus nerve ‘senses’ the inflammatory response in different organs of the body and reacts to it in the brainstem – without there being any actual infection of brain tissue,” Dr. Radbruch explains.
“We think it’s possible that if the inflammation becomes chronic, that could be what causes the neurological symptoms often observed in long COVID in some people,” Conrad says.
Social and Advocacy
Children and young adults with Long COVID are being sent to nursing homes because there are no medical support options in their homes.
https://twitter.com/LongCovidFam/status/1760835633285648680
Vaccines
Vaccine responses are better than previously reported and follow known B cell physiology.
2/22/24 Immunity: SARS-CoV-2-infection- and vaccine-induced antibody responses are long lasting with an initial waning phase followed by a stabilization phase https://buff.ly/3I8r4so
Vaccination antibody kinetics show two phases: an initial rapid decrease in SARS-CoV-2 spike IgG antibodies, followed by stabilization to at least 7 to 9 months.
The study agrees with known B cell physiology (plasmablasts initially make antibodies. Longer lasting antibodies made from long-lived plasma cells migrate from lymph nodes into the bone marrow.
Waning of antibodies was slower after the booster doses.
Key points:
COVID-19-vaccine-induced immunity wanes but stabilizes at an individual setpoint
Pre-existing immunity results in rapid antibody responses upon vaccination
Boosters equalize antibody titers between individuals with and without hybrid immunity
Antibody kinetics show two phases: an initial rapid decay followed by a steady state
2/19/24 Cell Host & Microbe (D. Ho lab): XBB.1.5 monovalent mRNA vaccine booster elicits robust neutralizing antibodies against XBB subvariants and JN.1 https://buff.ly/3T8gtUJ
Long COVID
https://twitter.com/EricTopol/status/1761061024097337751
2/22/24 Ground Truths by Eric Topol: Towards Solving the Long Covid Puzzle https://buff.ly/49NFKZA
https://twitter.com/thephysicsgirl/status/1760442621875585512

2/22/24 Science (Z. Al-Aly & Eric Topol): Solving the puzzle of Long Covid https://buff.ly/48oTkSd
Review of what we know about Long COVID, different subtypes of LC and LC prevention with vaccines and Paxlovid, Ensitrelvir and Metformin, as well as physical mitigations like better indoor air quality and masking when necessary.
Reinfections increase the risk of getting LC.
Finding treatments for Long Covid must be prioritized.
Leaky BBB and Long COVID
Long COVID ‘brain fog’ and cognitive problems including memory loss, difficulty focusing, and thinking, may be due to leaky blood-brain barrier as seen by dynamic contrast-enhanced MRI.
2/22/24 Nature Neuroscience (Dublin): Blood–brain barrier disruption and sustained systemic inflammation in individuals with Long COVID-associated cognitive impairment https://buff.ly/49rDJ5K
Damaged leaky blood vessels in the blood brain barrier (BBB) in people with Long COVID and brain fog.
Inflammation and persistent dysfunction (leakyness) of the blood brain barrier (BBB) in Long COVID contribute to cognitive dysfunction (brain fog).
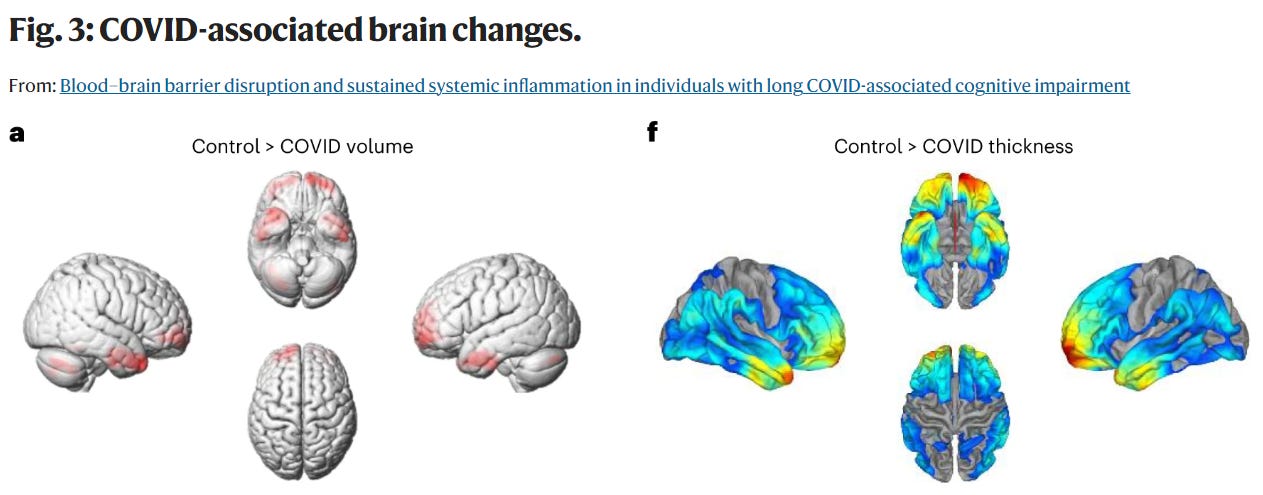
Brain regions with reduced volume in patients with previous SARS-CoV-2 infection.
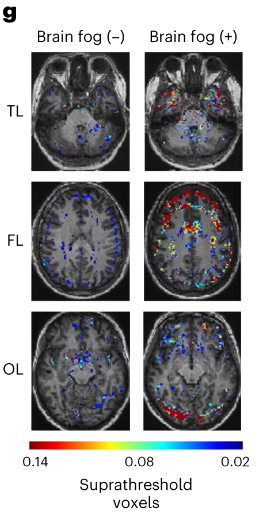
g, Representative BBB permeability maps at the level of the TLs, FLs and OLs showing enhanced BBB permeability in cases with brain fog.
Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) was used to measure the density, integrity, and leakiness of tissue vasculature.
This study shows that SARS-CoV-2 can cause white matter brain volume loss and leaky blood-brain barrier in some patients.
2/22/24 Trinity College Dublin: Trinity team discovers underlying cause of “brain fog” linked with Long COVID https://buff.ly/3ONTb40
My understanding: Leaky blood vessels in the blood brain barrier could allow toxic and inflammatory molecules into the brain, causing brain damage and brain fog.
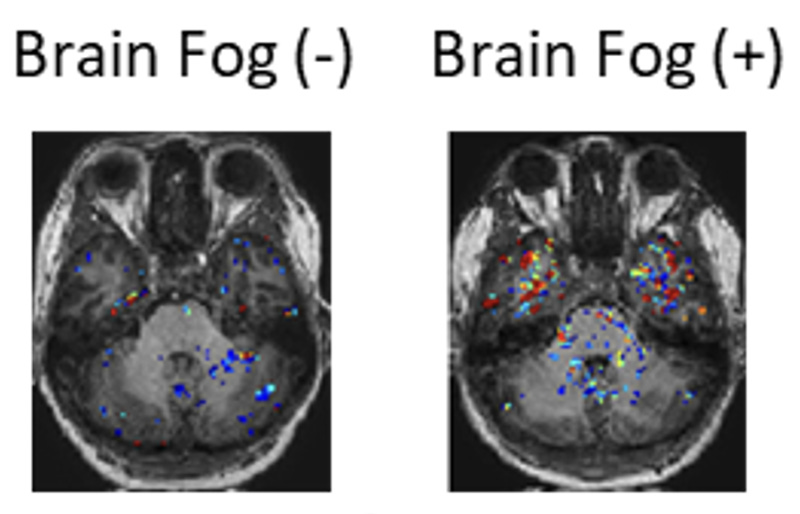
MRI scans in patients with Long-COVID with or without “brain fog”. Increased “leakiness” of the blood vessels is seen (here in the temporal lobe region of the brain) in those patients with brain fog (indicated by red signal).
2/22/24 Gen Engineering & Biotech News: Leaky Blood Vessels in the Brain Linked to Brain Fog in Long COVID Patients https://buff.ly/4bYJKZs
"Leaky blood vessels in the human brain, in tandem with a hyperactive immune system may be the key drivers of brain fog associated with Long COVID. This is critically important, as understanding the underlying cause of these conditions will allow us to develop targeted therapies for patients in the future,” said Matthew Campbell, PhD
Using dynamic contrast-enhanced MRI to identify the changes to neural vasculature showed reduced integrity of the blood vessels in Long COVID patients with brain fog and other cognitive impairments (memory loss, difficulty focusing, and thinking), compared with Long COVID patients without cognitive impairments.
2/22/24 PolyBio Research Foundation Grants announced
https://twitter.com/polybioRF/status/1760673645838614566
New LongCOVID research launched by PolyBio’s global consortium of scientists - PolyBio Research Foundation https://buff.ly/3I8uPOw
Most studies funded look at SARS-CoV-2 viral persistence and the impact of viral activity on Alzheimer’s & cardiovascular disease.
Icahn School of Medicine Mount Sinai, (Putrino): A clinical trial of repurposed HIV antivirals in LongCOVID https://buff.ly/48nDasd
A clinical trial to test if two repurposed HIV antivirals (Truvada and Maraviroc) can reduce symptom burden in patients with Long COVID.
UCSF: LIINC PASC Tissue Program: A multimodal assessment of the tissue-based virologic drivers of Long COVID https://buff.ly/4bR2Lgn
Yale: Molecular identification of SARS-CoV-2 RNA persistence https://buff.ly/3I8uQSA
French National Institute for Health & Medical Research/ESPOIRS: SARS-CoV-2 persistence and impact on Long COVID megakaryocytes & platelets https://buff.ly/49pKjJQ
U Mass Chan Med: Impact of SARS-CoV-2 infection on Alzheimer's and neurodegenerative disease https://buff.ly/3wpxErU
NYU: Deep characterization of SARS-CoV-2 cardiovascular reservoirs and plaque formation https://buff.ly/3UR3FmN
Karolinska Institutet Sweden: Genetic variants & restrained antiviral immunity in severe Long COVID https://buff.ly/3UQDKf3
UCSF: COVID-19 Post Sudden Death Autopsy Study https://buff.ly/49qPwBf
J. Craig Venter Institute: Deep characterization of antiviral immune responses and Long COVID pathogenesis https://buff.ly/3uHPmXa
Icahn School of Medicine at Mount Sinai: Lumbrokinase LongCOVID & ME/CFS clinical trial https://buff.ly/42NQp4e
University of Pennsylvania (Dr Sara Cherry, Maayan Levy, et al): Long COVID: Defining the viral RNA reservoir in the gastrointestinal tract https://buff.ly/4bKBTOZ
J. Craig Venter Institute: Long COVID oral cavity biomarker study https://buff.ly/3TboRTv
Karolinska Institutet Sweden: Impact of SARS-CoV-2 on Long COVID gut and lymphoid pathology https://buff.ly/48u7DFh
University of Pennsylvania (EJ Wherry lab): Second phase expansion of LongCOVID T cell & lymph node analysis https://buff.ly/3wjE3on
J. Craig Venter Institute: Mechanistic biomarker discovery of LongCOVID endotypes https://buff.ly/49mOw15
The OSLUV Project/Icahn School of Medicine at Mount Sinai: LongCOVID clinic clean indoor air initiative https://buff.ly/3OUeAsl
Icahn School of Medicine at Mount Sinai: LongCOVID open medical education program https://buff.ly/3UQDY5T
https://twitter.com/Em23397/status/1760724011024105791
2/22/24
https://twitter.com/postviraltrials/status/1760864796151324748
IFN-γ as a biomarker for Long COVID
2/21/24 Science (Cage): Spontaneous, persistent, T cell–dependent IFN-γ release in patients who progress to Long Covid https://buff.ly/3OTTDOd
Persistently elevated interferon-gamma (IFN-γ) from peripheral blood mononuclear cells (PBMCs) after COVID infection may be a biomarker for Long COVID.
The authors detected persistently high levels of interferon-γ (IFN-γ) from peripheral blood mononuclear cells (PBMCs) of patients with Long Covid using highly sensitive FluoroSpot assays.
The IFN-γ release was CD8+ T cell–mediated and dependent on antigen presentation by CD14+ cells.
Resolution of Long COVID symptoms was associated with IFN-γ decreasing to baseline levels.
Persistent COVID infections are also seen in the general population and not only in immunocompromised people.
2/21/24 Nature (Oxford): Prevalence of persistent SARS-CoV-2 in a large community surveillance study https://buff.ly/3OV33sG
93,927 high-quality sequenced samples from November 2020 and 15 August 2022.
0.1–0.5% of COVID infections become persistent with typically rebounding high viral loads and last for at least 60 days.
High viral loads suggest actively replicating virus. Some viral mutations are noted over time.
People with persistent SARS-CoV-2 infections had more than 50% higher odds of reporting Long COVID.
2/21/24 Nature: Deep phenotyping of post-infectious myalgic encephalomyelitis/chronic fatigue syndrome (PI-ME/CFS) https://buff.ly/3UNabLx
Small study: 17 people PI-ME/CFS vs. 21 healthy volunteers
PI-ME/CFS decreased functional status that was 1.5 to two standard deviations worse than the general population.The fatigue of PI-ME/CFS is due to decreased activity of the right temporal-parietal junction causing dysfunction of integrative brain regions that drive the motor cortex.
Dysregulation of catecholamine synthesis noted.
T cell exhaustion, seen by elevated PD-1 in cerebrospinal fluid (CSF).
Autonomic dysfunction with increase in sympathetic and a decrease in parasympathetic activity in PI-ME/CFS that affected HRV.
Sex differences in PI-ME/CFS in:
immune system responses including different gene expression in peripheral blood mononuclear cells (PBMCs)
muscles. Both males and females PI-ME/CFS samples had increased oxidative stress, but by different pathways.
CSF metabolites
PI-ME/CFS shows distinct sex differences in immune and metabolic dysregulation which suggest persistent antigenic stimulation.
Summary slide:
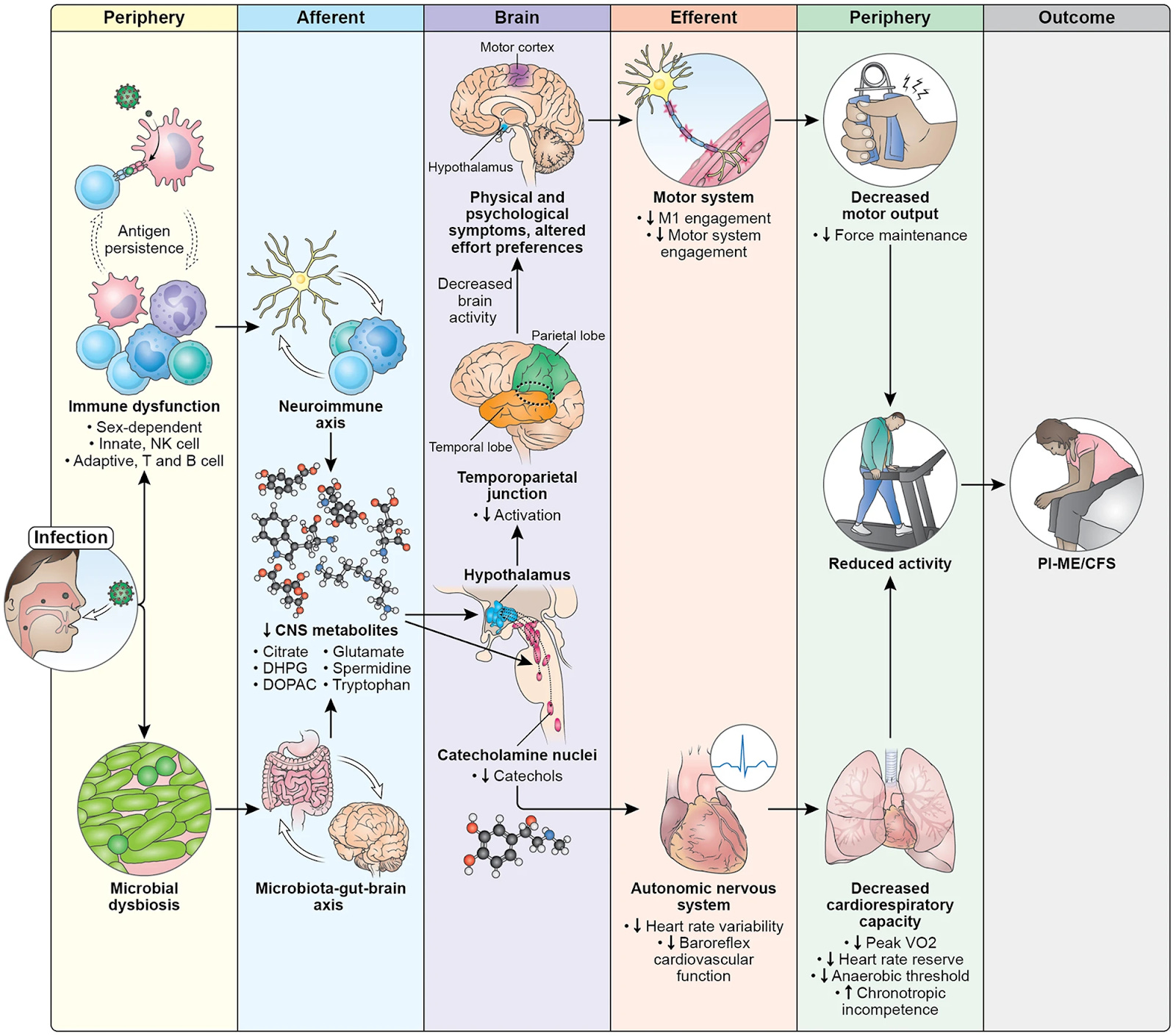
PI- ME/CFS potential mechanisms:
Exposure to an infection leads to immune dysfunction and changes in gut microbiome.
Immune dysfunction (from antigen persistence of pathogen) affects both innate and adaptive immune systems that are sex dependent.
These immune and microbial alterations impact the brain, leading to decreased concentrations of metabolites which impacts brain function.
The catecholamine nuclei release lower levels of catechols, which impacts the autonomic nervous system and manifests with decreased heart rate variability and decreased baroreflex cardiovascular function, with downstream effects on cardiopulmonary capacity.
Altered hypothalamic function leads to decreased activation of the temporoparietal junction during motor tasks, suggesting a failure of the integrative brain regions necessary to drive the motor cortex.
This decreased brain activity is experienced as physical and psychological symptoms and impacts effort preferences, leading to decreased engagement of the motor system and decreases in maintaining force output during motor tasks.
Both the autonomic and central motor dysfunction result in a reduction in physical activity. With time, the reduction in physical activity leads to muscular and cardiovascular deconditioning, and functional disability.
2/21/24 USA Today: Young adults (age 25 to 49) have higher rates of long COVID than older Americans: See the charts https://buff.ly/49nAVq5
2/19/24 Annals of Epidemiology: The impact of COVID-19 vaccination prior to SARS-CoV-2 infection on prevalence of long COVID among a population-based probability sample of Michiganders, 2020-2022 https://buff.ly/3OVmz8l
"Long COVID prevalence was 40-60% lower among adults vaccinated (vs. unvaccinated) prior to their COVID-19 onset."
2/21/24 Washington Post: Tax records reveal the lucrative world of COVID misinformation https://buff.ly/48r5wlq
Four “nonprofits” that spread of medical misinformation collectively received more than $118 million between 2020 and 2022, “enabling the organizations to deepen their influence in statehouses, courtrooms and communities across the country.”
Children’s Health Defense, an anti-vaccine group founded by Robert F. Kennedy Jr., received $23.5 million in contributions, grants and other revenue in 2022 alone.
Informed Consent Action Network, anti-vaccine group, nearly quadrupled its revenue during that time to about $13.4 million in 2022.
Two other groups, Front Line Covid-19 Critical Care Alliance (FLCCC) and America’s Frontline Doctors, went from receiving $1 million combined when they formed in 2020 to collecting more than $21 million combined in 2022, according to the latest tax filings available for the groups.
Half of those gifts over $100,000 were made through a tax vehicle popular among the ultrawealthy known as “donor-advised funds,” which allow individuals to obscure their identities.
It is sick how much money each of these individuals received from the 4 groups to spread misinformation and lies about COVID and its treatment.
AI:
2/20/24 Nature: Generative AI’s environmental costs are soaring — and mostly secret https://buff.ly/48nYM7R
Other news:
2/22/24 NBC news: Three Alabama clinics pause IVF services after court rules that embryos are children https://buff.ly/3SLMCQu
The Alabama Supreme Court ruled that embryos created through in vitro fertilization (IVF) are considered children.
https://www.threads.net/@hillaryclinton/post/C3qIPyaxZZv

2/19/24 Nature: A terminal metabolite of niacin promotes vascular inflammation and contributes to cardiovascular disease risk https://buff.ly/3I5YMi7
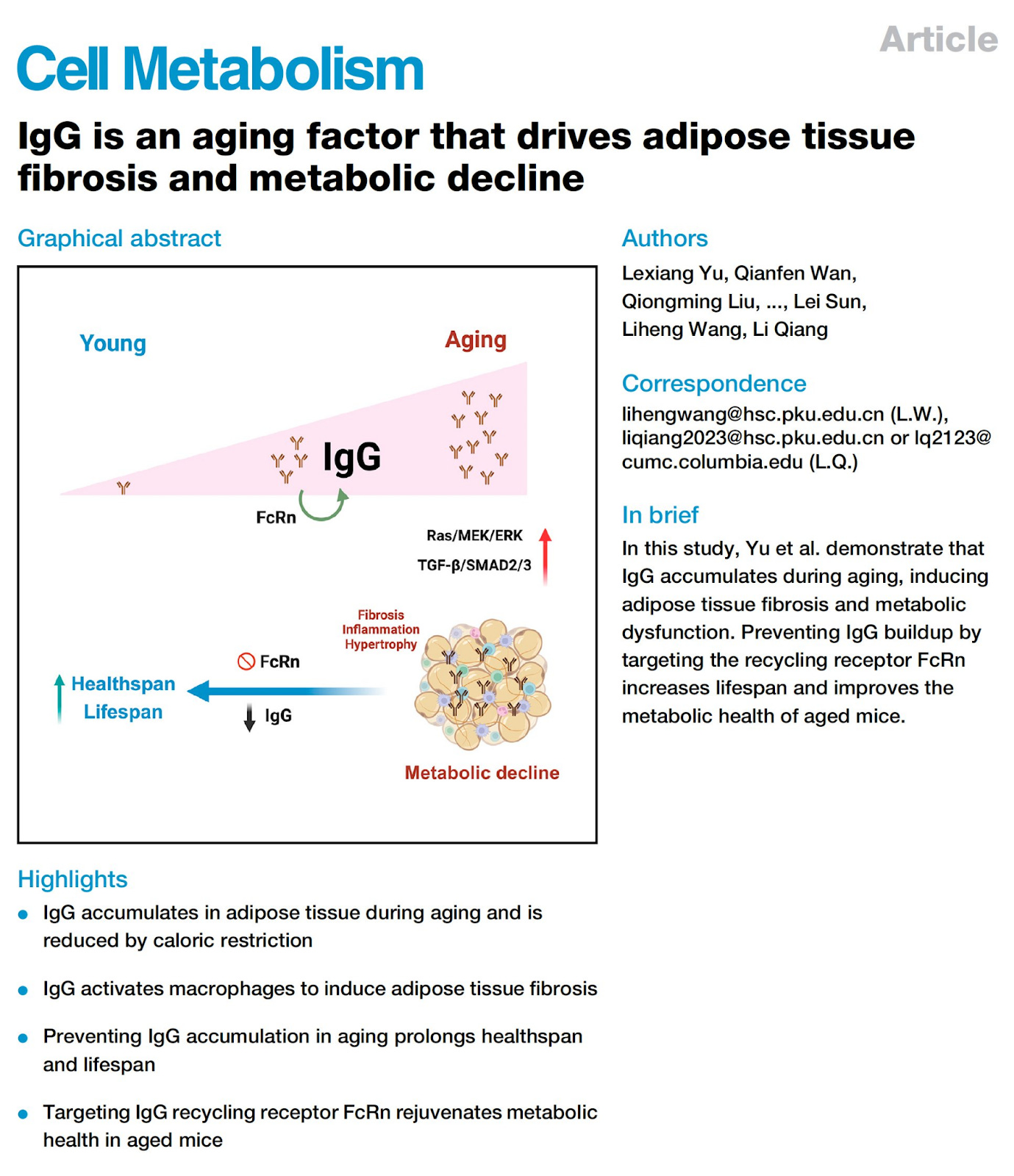
2/19/24 Cell: IgG is an aging factor that drives adipose tissue fibrosis and metabolic decline https://buff.ly/48hQGhf
CNN: Japan’s newest species is a tiny, panda-like sea creature https://buff.ly/48vK0w2
The skeleton panda sea squirt


Thank you!!
Dr Ruth,
Thank you so much for sharing your absolutely excellent resources, and doing that in near lay language.
I would encourage you to look more at the immunity issues and the fading of immunity over time. This is an area where you far exceed many of your colleagues.
Many RNA viruses mutate, hybridize or re-assort so rapidly that mammalian physiology has learned in some way that we do not yet understand to recognize that and to then change immune response.
For SARS-CoV-2, our bodies recognize that building last immunity is not beneficial. Doing so is an energy and resource burden. But, the virus will soon mutate and hybridize to defeat that built immunity. As a result, our immune systems mount a two stage adaptive defense.
First is the production of antibodies tailored to attack the invader (infection or vaccine derived materials). This builds quickly and then fades slowly at a constant rate plotted logarithmically. The strength of the response is to a degree dose (or insult) dependent. That plateaus at some point. So vaccines can be highly effective on a par with immunity built from infection. However, as we saw in the bivalent vaccine, if the dose of vaccine is lower, the strength and durability of the response can be lower as well.
For most of the vaccines, they were well targeted to circulating strains. And they produced strong immunity that started at about 95% against any disease or transmission. This fades relatively rapidly to drop below about 50% by 4-5 months after vaccination.
Simmilarly, immunity from infection lasts about as long.
Second though, the body then also produces B and T memory cells to the insult. These serve as a reminder of the infection allowing rapid reproduction of that immunity to those strains. This immunity also fades in much the same way and it too is essentially gone at 6-9 months.
In both cases there is no firm cutoff. The response becomes less and less as time passes.
After these, the virus has mutated sufficiently that the old immune response is insufficient to fight the new strains. And then the body mounts a new defense and builds new immunity. That too then fades as before. Rinse and repeat.
The mainstream for reasons I cannot fathom seems unwilling or unable to believe or accept this. It seems that they may be caught in simpler ideas, despite knowing better. These ideas seem rooted in experience of DNA virus immunity that often lasts a lifetime, or nearly so. And too of the flu, an RNA virus that has a lower reproduction number and that as a result is limited to epidemic phases when people move indoors and aggregate in the winter.
The immune memory for flu virus does seem to last longer. And so immunity to past versions similar to the current versions tend to trigger some degree of protection. However, this is still viewed as being caused not by immunity fading, but instead by the virus re-assorting and mutating away sufficiently that the old immunity is not effective. This holds at its core the mistake of believing that the immunity is long term or permanent and not recognizing the strategies employed by the body to conserve precious resources and intentionally forgetting the old invaders - since they are unlikely to come around again.
With SARS-CoV-2, in early 2020 when the virus first arrived in Washington State (and elsewhere), it showed growth rates in the population (which was taking few or no precautions) such that the growth was about 35% per day. It had an R0 of about 15. In China at the same time, huge efforts there to contain the virus had begun and the reported R (not R0 as incorrectly assessed) was about 3-7.
The case fatality rate varied a lot based mostly on differences in age distributions. The CFR on average was about 4.5%. In Italy where it rampaged through communities of elderly folks, the CFR was around 18%. The CFR for the Wu-1 strain showed a straight linear relation to age plotted logarithmically, meaning that people over about age 55 was at risk with exponentially increasing risk of death with increasing age. Those under 55 were also at risk, but statistically at a lower rate.
What this actually showed was the shift from primary reliance on adaptive (antibody based) immunity in the young to primary reliance on innate (cytokine derived) immunity in the old, as the adaptive immune response fades with age.
That continued through the AY (Delta strains).
Then came Omicron (rodent - likely mouse derived) strains, when the pandemic in some unidentified animal reservoir (most likely mice) jumped to humans in at least five variations (BA.1, BA.2, BA.3, BA.4, and BA.5). In passing through mice (or whichever species it was) and adapting to them, the virus seems to have shifted its attack to rely more on TMPRSS2 and less on ACE2.
The practical result was that the virus became better at attacking the sinuses and upper respiratory tract, and less on the lungs. Though both still occur. The virus is now known to leverage attack on at least 15 cell surface receptors. In doing this, the lethality dropped by at least a factor of 10. Though that did not change the other impacts through complimentary immune system damage and clotting, spike protein toxicity to the cardiovascular system, heart, brain stem and organs, or to immune system damage leading to an AIDS like decline in CD8, long COVID, and hyper accelerated aging through methylation of the DNA, truncation of the telomeres, and the afore mentioned organ and brain damage.
At the same time, a fiction circulated that viruses "aways get weaker". This is not true. But coinciding as it did with the decline in immediate lethality and the also competing idea of "herd immunity", it set the stage for governments to decide that it was both too hard to fight the virus, and too costly in its impacts on business. And so now we are caught in a "three monkeys syndrome" of denial.
What this conceals is ever increasing risks of hybridization with the virus circulating in pandemics in other species, wild type cousins in pandolins, camels, and bats (plus others) that are extremely lethal, or the on-going hybridization and mutation toward immune evasion.
It also conceals the immense impacts on health care both now, and the hidden impacts that are growing from long COVID, immune destruction, and aging that may collapse society in the near future as those impacts grow.
What is needed are changes in understanding by the experts to recognize the way the immune system chooses to forget this virus, and the impacts that have, which necessitate continual revision of vaccines on an at least twice annual basis, and allowing for vaccination not less than twice a year (to protect against severe disease and death), or better three times a year (to protect against infection and long COVID, immune damage and aging.
In many ways, the accumulated population level harm form 3 or more infections and recoveries is already sealed in. And that will have profound societal impacts over the next several years. However, the impacts are still growing, and we need to take action to protect those not yet destined to such difficulties.
We also need to recognize that it isn't just those who are immunodeficient that are at heightened risk. So too are those with hyperactive immune response (autoimmune disease). Every infection carries with it a 13-14% chance of developing a new autoimmune disease and an equally large risk or reactivating autoimmune diseases. And since people with long term autoimmune disease often have 6 or 7 different autoimmunities, the risk for them is near unity of some autoimmune problem developing with each infection. That is currently unrecognized.
Please do continue to do your incredibly good work. It is vital.
Oh - and back to the beginning, the 54% immunity that the vaccines provide against JN.1 is helpful. It is not lasting. Based on prior experience, that level of immunity provides at best 3 months of protection against disease and perhaps 4 against severe disease and death. Though it is better than nothing, it is NOT durable immunity. It is NOT success. It is instead a sign of a vaccine that is now all but ineffective against the current strains and the need for a new vaccine targeted at the JN.1.x derived strains - NOW. By the fall, JN.1.x will be a memory having been replaced by some new variant or hybrid and its progeny. Even newer vaccines will need to be in process then to target those in an unending cascade.
And that is another mark and indicator of the failed ideas that our leaders are using to guide their now nearly complete lack of response to the pandemic.
Another indicator is the loss of nearly all data and information about the pandemic. Though this aids in trying to get people back to work and shopping, and the near-term economic issues, in the longer intermediate term, these are catastrophic approaches.