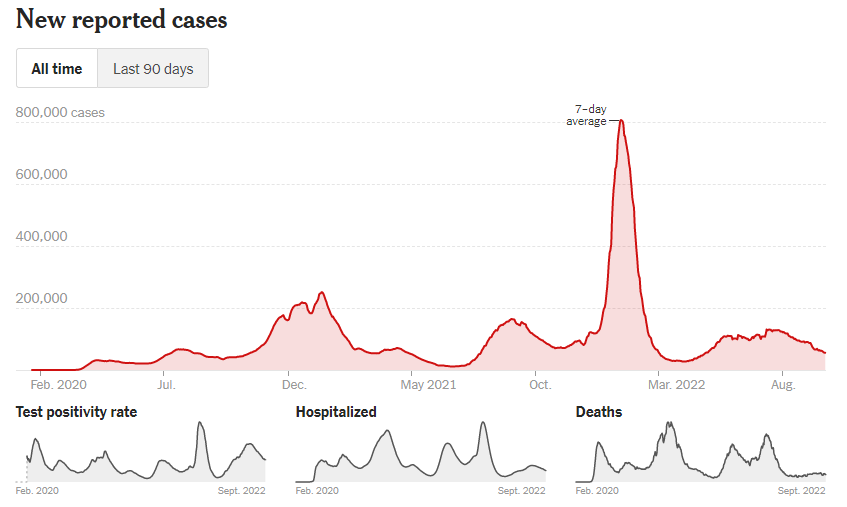
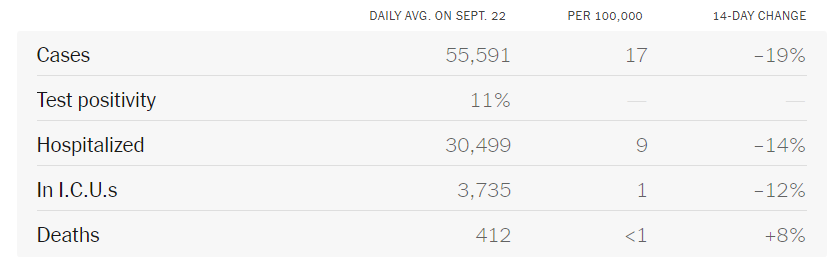
This week, President Biden announced on 60 Minutes that "The pandemic is over. We still have a problem with COVID. We are still doing a lot of work on it. But, the pandemic is over." First of all, the pandemic is not over. There are more than 55,000 new reported cases per day (and the real number is probably 5x this since most people are doing home testing now if they do testing). More than 400 people are dying from COVID every day. Millions of people have Long COVID and chronic conditions appearing after COVID infections. There are new variants that may outcompete BA.5 on the horizon. Cases and hospitalizations are now increasing again in the UK. The pandemic is not over, even though we all wish it were.
The new bivalent boosters that include Omicron BA.5 mRNA are available and it is recommended that all people age 12 and over get the booster. If you had a recent monovalent booster with the original virus mRNA, you should wait 2 months to get the bivalent booster. If you had a recent COVID infection, you should wait until 3 months to get the new bivalent booster. ACOG also updated their website recommending that pregnant people should get the new bivalent booster. It is easy to find locations that have the bivalent boosters available near you athttps://www.vaccines.gov/search/.
The President's statement about the pandemic being over is not going to help get the message out that all people age 12 and over should get the new bivalent booster. Although the boosters are not perfect, they have been shown in many studies to protect against severe COVID infections and death. They also help to decrease your risk of Long COVID by 15 to 50% depending on the study. It appears that there may be several new variants on the horizon which may outcompete BA.5 and could possibly cause a new wave. The bivalent booster should protect against these better than the original vaccines as the bivalent booster protects against Omicron BA.4/5.
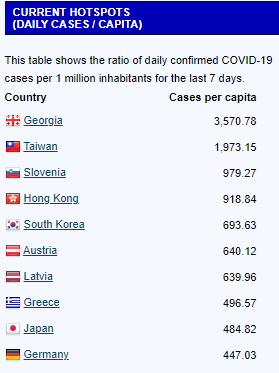
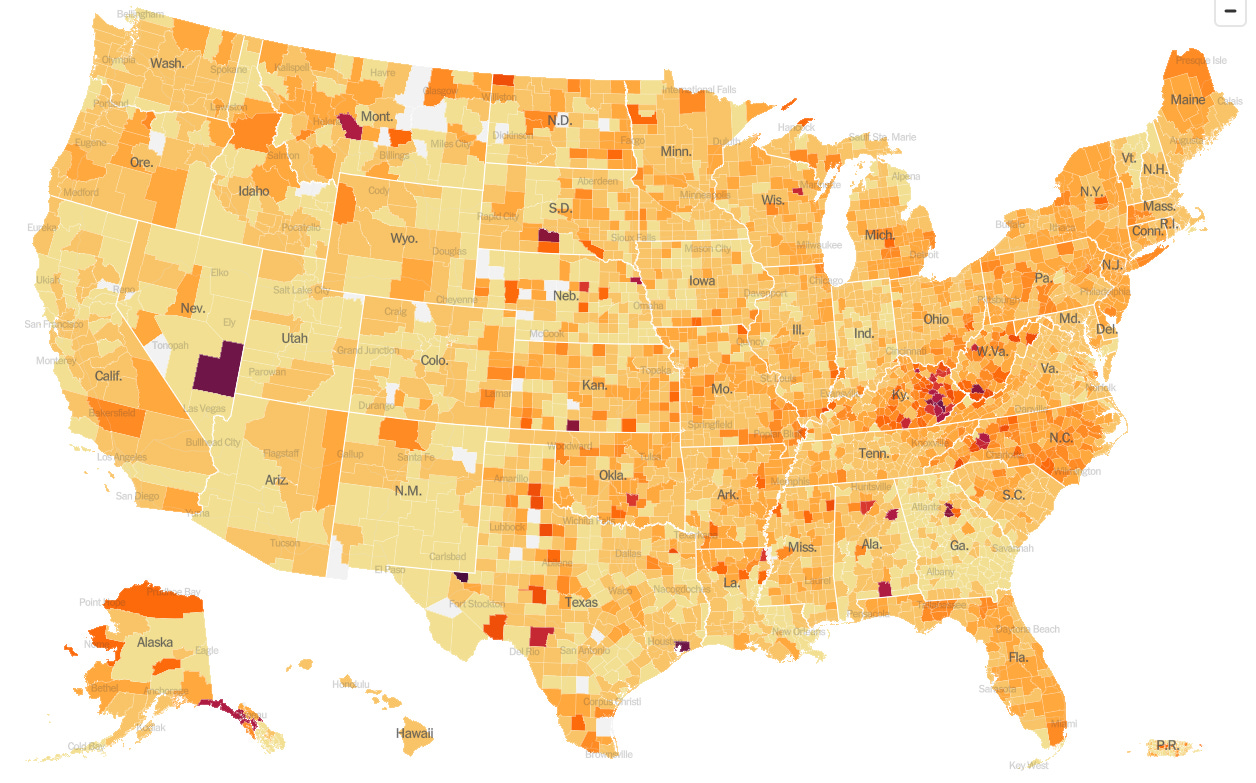
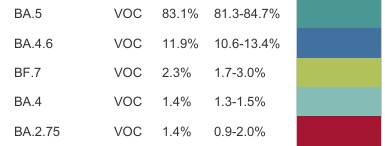
There are several new variants that scientists are now watching. BA.2.75.2 has picked up 3 new mutations and it is increasing 9.4% per week in the UK relative to BA.5. Variant BQ.1.1 may soon outcompete BA.5 in the UK as its growth is noted to be 19.7% higher than BA.5. Studies of wastewater here in the U.S. show some new cryptic lineages including BU.1 and BQ1.1 which have 4 and 5 more mutations than BA.5 respectively. Variant BF.7, another descendent of BA.5, has been increasing in wastewater samples in the last 2 weeks in the United States although it is only at about 2 to 3% of variants seen in the US at this point. The virus continues to mutate and evolve in order to evade our immunity wall. It is not certain that any of these variants will cause a new wave, but it is possible.
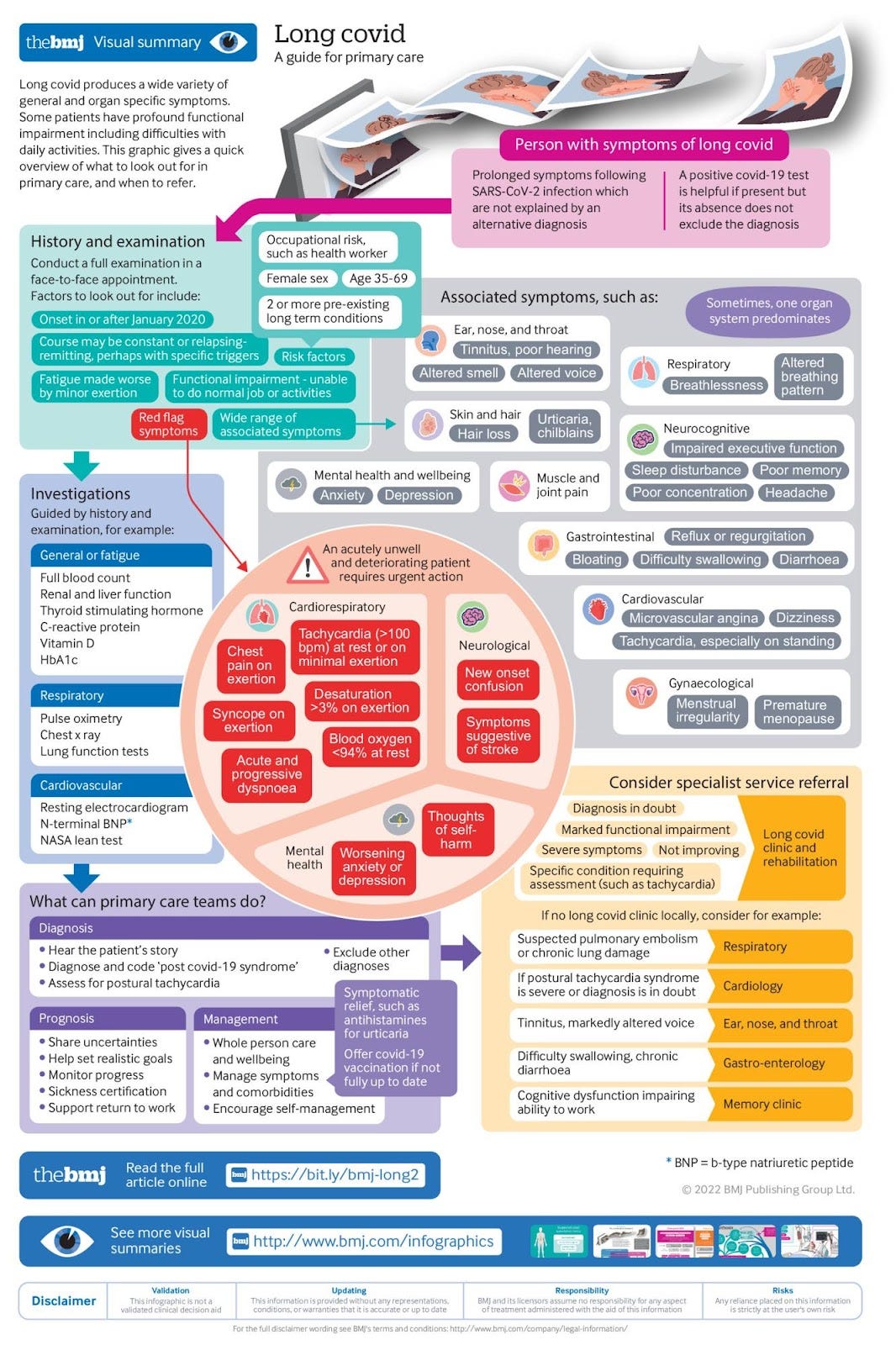
There were several articles on Long COVID this week. Trish Greenhalgh et al. put out a detailed article yesterday in the BMJ with Long COVID resources for patients and for primary care healthcare providers. Included are links to eLearning modules and other online resources. The WHO updated their living document Clinical management of COVID-19 to include a new Chapter 24 that gives rehabilitation recommendations for treating Long COVID. The WHO has 2 other living guidelines that are updated when new evidence is available- Drugs to prevent COVID-19 and Therapeutics and COVID-19. Time magazine ran an article called "Long COVID Experts and Advocates Say the Government Is Ignoring 'The Greatest Mass-Disabling Event in Human History'" which is worth a read.
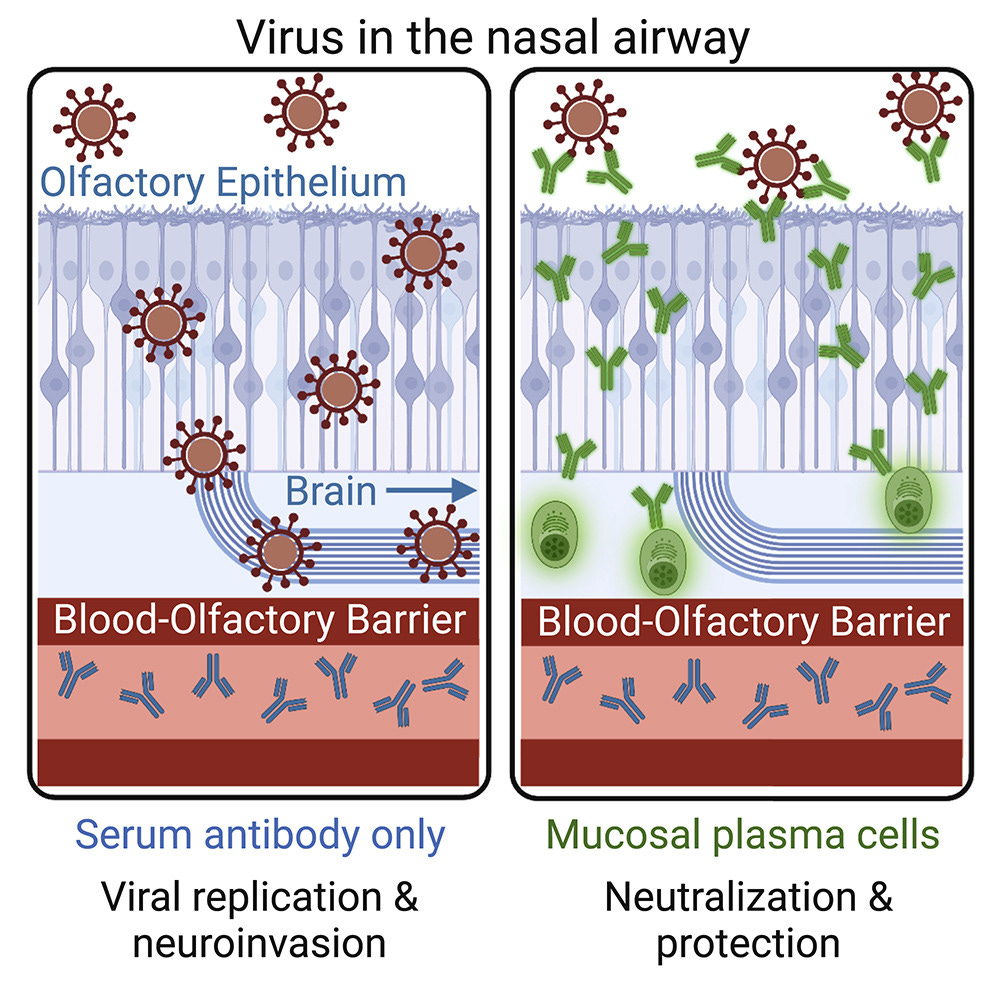
A new report from the Veterans Administration shows that about 7% of veterans who had COVID developed a new neurologic disorder such as stroke, memory and cognition problems, migraines, etc. one year later. The neurologic problems were significant, but because the infections happened before January 2021, <1% of people in the study were vaccinated and the data is from pre-Omicron infections in a veterans population which skews more to older white males. In a different study on neuroinflammation, researchers reported their discovery of a blood-olfactory barrier that keeps serum antibodies away from nasal epithelial cells. SARS-CoV-2 can go from the nose (via olfactory epithelium) to the brain and cause brain inflammation unless there are local olfactory plasma cells making antibodies within the nasal mucosal tissues. Abnormal cortisol levels and disturbance of the hypothalamus-pituitary-adrenal axis in people with Long COVID may be related to brain inflammation. Nasal booster vaccines could increase nasal IgA antibodies which could stop the SARS-CoV-2 virus from entering the body.
Three percent of people are homozygous for an APOE gene. A new study in Nature magazine shows that mice with APOE4 or APOE2 genes had worse COVID outcomes including an increase in death. APOE3 mice did the best with COVID infections. In humans, the UK Biobank shows that people with APOE4 gene mutations have worse outcomes from COVID as well. APOE4 tends to increase the risk of Alzheimer's disease in humans, APOE2 decreases that risk. APOE genes can also affect risks of atherosclerosis and anti-tumor immunity.
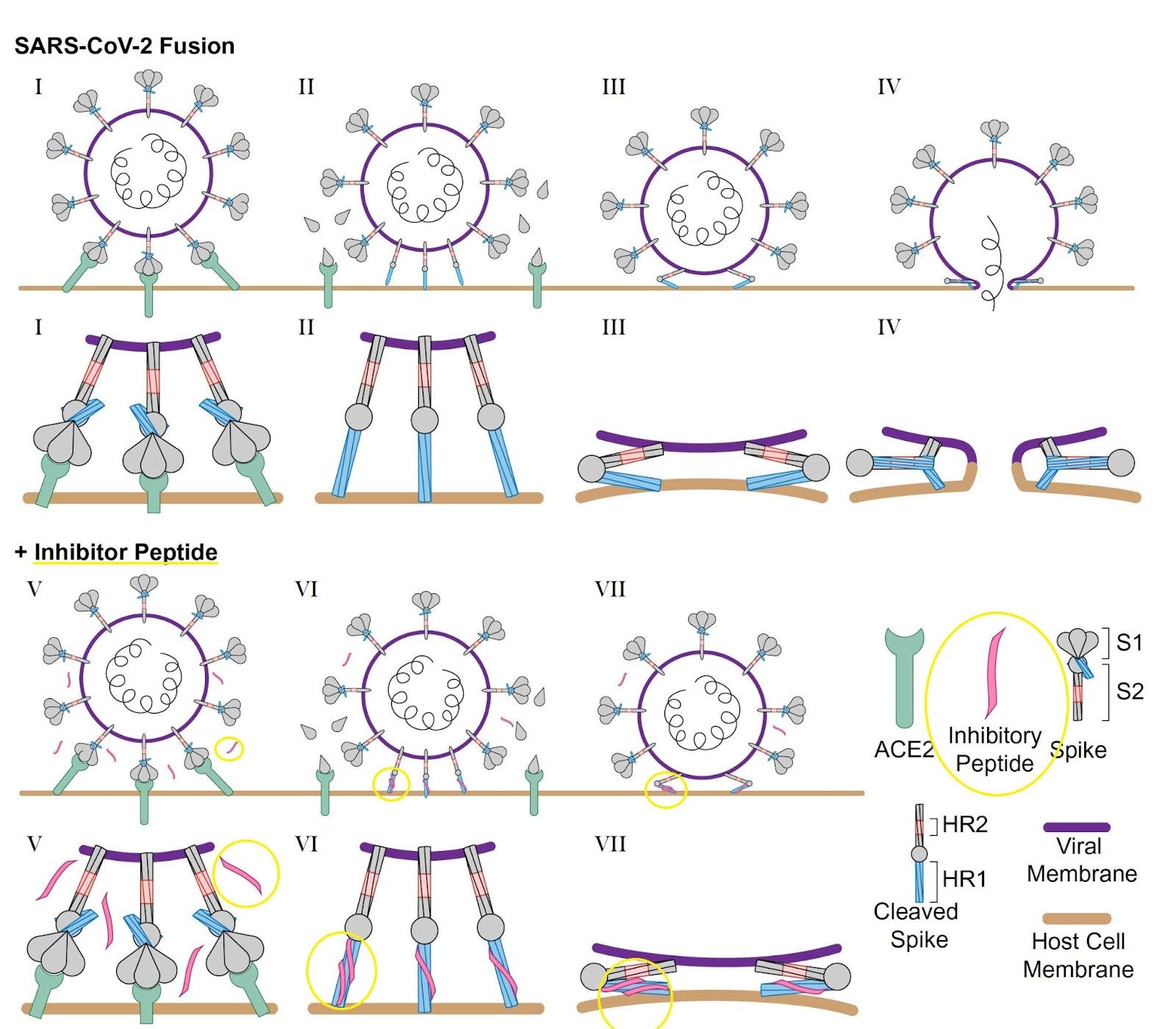
And finally, some good news. This week, a group from Stanford announced that they have discovered a simple peptide that inhibits infection by all major variants of SARS-CoV-2 with nanomolar efficacies. @JasperLope from Twitter explains: “[My] very unscientific explanation: They have developed a special "hug molecule" [the Inhibitory Peptide] that keeps Covid from being able to do anything by tangling up its “grabby parts”.
There is also a new global initiative to address Long COVID called The Long Covid Research Initiative (LCRI) which has gathered research teams from top universities to work together to discover treatments for Long COVID. The LCRI is privately funded so there is less bureaucracy. Their focus will be on viral persistence (viral reservoirs) of SARS-CoV-2 causing Long COVID. Candidate therapeutics include antivirals and immunomodulators.
Thanks for reading Dr. Ruth’s Newsletter! Subscribe for free to receive new posts and support my work.
9/23/22 Health Advisory Santa Clara County:
1. COVID-19 and Influenza
COVID and Influenza: Although laboratory-reported COVID-19 case counts are declining, community transmission of COVID-19 remains significant, as evidenced by wastewater data. In addition, the newest emerging variants of concern (BA.2.75 and BF.7) have been detected in Santa Clara County. Increases in indoor and travel-related transmission are anticipated this winter.
Due to changes in masking policies and other factors, influenza activity is also anticipated to be higher this season than 2020 or 2021.
Provider Updates:
Indoor masking continues to be strongly recommended in public settings and required in high risk settings in Santa Clara County, independent of state masking requirements.
Both Pfizer and Moderna COVID-19 bivalent booster vaccines are now widely available.
Cases of Monkeypox (MPX) are now decreasing globally, nationally, and locally. Transmission continues to be primarily among men who have sex with men (MSM).
3. West Nile Virus
Situational Update: As of 9/16/22, there have been 54 human cases of WNV in California.
In Santa Clara County, increased West Nile Virus activity has been detected in both mosquitoes and birds, particularly in the Northern part of the county (Sunnyvale, Mountain View, and Los Altos Hills).
WNV should be considered in any person with a febrile or acute neurologic illness who has had recent exposure to mosquitoes, blood transfusion, or organ transplantation. Severe WNV can present as meningitis, encephalitis, or acute flaccid myelitis (like polio).
4. Acute Flaccid Myelitis (AFM)
Situational Update: Prior to COVID pandemic, there have been periodic surges in late summer and early fall of enterovirus D68 (EV-D68) (the virus most commonly associated with AFM cases), followed by surges in AFM in subsequent weeks. In August 2022, an increase in EV-D68 respiratory disease was detected in sentinel surveillance sites in the United States, including California, raising concern for a surge in AFM cases in coming weeks.
9/22/22 Fierce Healthcare: New COVID-19 variant's spread draws concern from CDC https://buff.ly/3BJk2a5
BF.7 and BA.2.75.2 are being watched.
In the last two weeks the BF.7 has doubled its incidence nationally from 0.8% to 1.7%. The largest growth has been in the Northeast United States, Region 1, where the incidence is now over 3%.
9/22/22 BMJ, Trisha Greenhalgh et al: Long Covid—an update for primary care https://buff.ly/3dAlhQA
Long COVID: Resources for patients
Books
The Long Covid Self Help Guide 37—written by specialists at a long covid clinic offering lay explanations and self-management strategies for the different symptom clusters of long covid
Support for rehabilitation: self-management after COVID-19 related illness—a World Health Organization guide for patients20
Physiotherapy for Breathing Pattern Disorders https://www.physiotherapyforbpd.org.uk —a patient facing site designed and run by specialist physiotherapists
Long covid physio: a resource site intended mainly for physiotherapists and their patients, set up by physiotherapists who have (had) long covid. https://longcovid.physio
9/22/22 Science (Stanford): SARS-CoV-2 infection drives an inflammatory response in human adipose tissue through infection of adipocytes and macrophageshttps://buff.ly/3dCn1ZK
SARS-CoV-2 can infect adipocytes and macrophages in adipose tissue.
COVID-19 severity could be affected by:
replication of virus within adipocytes
induction of local and systemic inflammation driven by infection of resident macrophages.
Adipocytes may be a reservoir of virus in Long COVID.
9/8/22 Introducing a Global Initiative to Address Long Covid:
World-class research teams (including Harvard, Stanford, UCSF, Johns Hopkins, Yale, Cardiff) working together to create a comprehensive, collaborative research program on Long COVID.
$15M+ in private funding. Less bureaucracy.
Focus is on viral persistence (viral reservoirs) of SARS-CoV-2 causing Long COVID.
Our clinical trials program will translate the findings of the research program into a pipeline of potential therapeutics to be used in clinical trials. Currently in early planning, candidate therapeutics include antivirals and immunomodulators.
An operating model with the urgency and pragmatism of a startup. LCRI brings cross-institution collaboration, an innovative trials program, and high levels of patient engagement.
Cohorts enrolled before January 2021, so <1% were vaccinated. Data is pre-Omicron.
Long Covid neurologic outcomes at 1 year from >150,000 people compared to > 11 million controls.
At 12 months following acute SARS-CoV-2 infection, there was increased risk of stroke, cognition and memory disorders, peripheral nervous system disorders, episodic disorders (for example, migraine and seizures), extrapyramidal and movement disorders, mental health disorders, musculoskeletal disorders, sensory disorders, Guillain–Barré syndrome, and encephalitis or encephalopathy.
In this study of 11.6 million people: 154k with COVID-19, 5.6 million contemporary controls, and 5.8 million historical controls
Even mild COVID-19 can lead to serious neurologic consequences.
The risk was increased 42%
This translated into 7 cases per 100 individuals with COVID-19.
These risks were evident regardless of age, race, sex, and health characteristics.
Younger adults had increased risks of memory and cognitive disorders, sensory disorders and disorders including Guillain–Barré and encephalitis or encephalopathy.
Equally troubling is the stronger effect of COVID-19 on mental health disorders, musculoskeletal disorders and episodic disorders in older adults, highlighting their vulnerability to these disorders following SARS-CoV-2 infection.
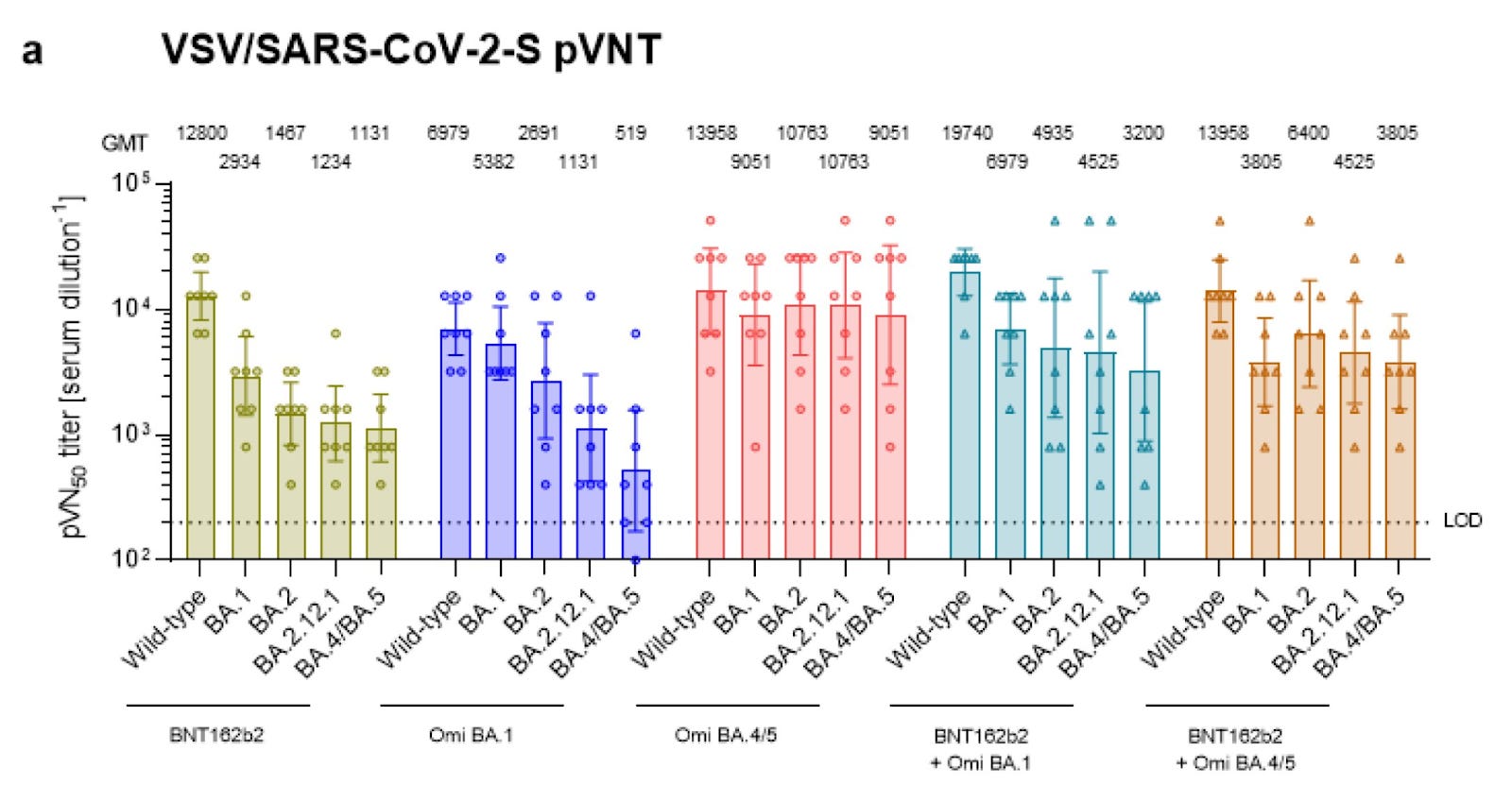
9/22/22 BioRxiV (BioNTech paper): Exposure to BA.4/BA.5 Spike glycoprotein drives pan-Omicron neutralization in vaccine-experienced humans and mice https://buff.ly/3qXNHHh
Neutralizing antibody data for BA.1 and BA.5 boosters, monovalent or bivalent, in mice.
BA.5 booster was better than BA.1 (for BA.5 counter).
Monovalent BA.4/5 booster elicited broad Omicron neutralization better than the bivalent booster.
9/21/22 Reuters: U.S. CDC expects bivalent Omicron COVID boosters for kids 5 to 11 by mid-October https://buff.ly/3SIz5aX
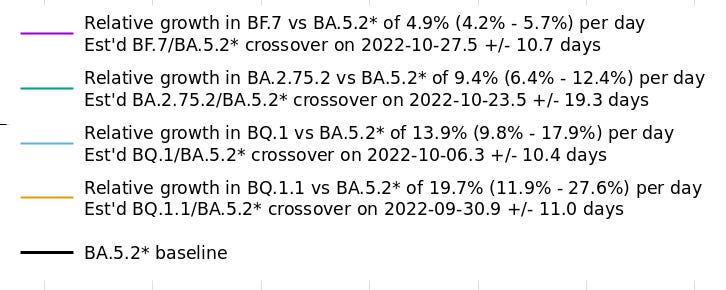
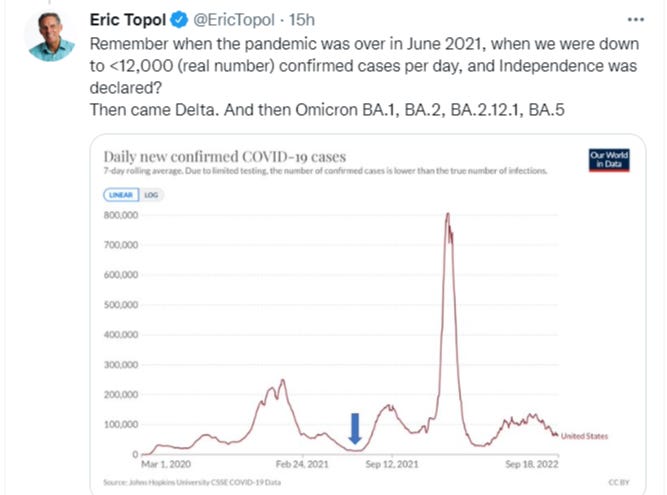
9/21/22 Eric Topol MD: Here is a graph showing the current growth advantage of BQ.1.1 and BA.2.75.2 relative to BA.5.2* in the UK: https://buff.ly/3BE9Yih
Using mathematical calculations:
BQ1.1 grows 19.7% faster than BA.5.2, expect crossover on 9/30/22. (+/- 9 days).
BQ.1, 13.9% faster, crossover on 10/6/22 (+/- 10 days).
BA.2.75.2, 9.4% faster, crossover on 10/23/22 (+/- 19 days).
9/21/22 Cell: Mucosal plasma cells are required to protect the upper airway and brain from infection in mice https://buff.ly/3SiWmjg
The newly discovered blood-olfactory barrier keeps serum antibodies away from the nose and nasal epithelial cells.
Without olfactory plasma cells making local antibodies in the nose, SARS-CoV-2 can go from the nose (via olfactory epithelium) to the brain and cause brain inflammation.
Nasal vaccines induce plasma cells in the nose which make antibodies that stop the virus from entering the brain via the nose.
CD4+ T cells and CXCR3 are also needed for local nasal immunity.
Eric Topol MD: “Yet another important reason to aggressively go after achieving mucosal immunity via nasal or oral vaccines.
Neuro-inflammation is an underpinning for many of the symptoms of Long Covid, including hypothalamus-pituitary-adrenal (HPA) axis dysfunction.”
9/21/22 MedRxiV: Liquid biomarkers of macrophage dysregulation and circulating spike protein illustrate the biological heterogeneity in patients with post-acute sequelae of COVID-19 (PASC, Long COVID) https://buff.ly/3R4T7uX
Evidence of immune dysregulation and persistence of viral protein in PASC.
Heterogeneity of these needs correlation with clinically defined PASC subtypes.
"pronounced dysregulation in almost all tested soluble factors including both pro-inflammatory and pro-fibrotic cytokines," eight months after infection.
9/21/22 Nature: Common human genetic variants of APOE impact murine COVID-19 mortality https://buff.ly/3Lzn3Or
Mice with APOE2 (protects against Alzheimer’s) or APOE4 (increased Alzheimer’s risk) had rapid COVID progression and increased mortality compared to mice with the APOE3 allele.
APOE3 mice did best with COVID, especially for male mice.
APOE variants act through (at least) two mechanisms: modulating viral infection and modulating antiviral immunity.
In humans, UK Biobank data shows people with APOE4 adverse COVID infection outcomes relative to APOE3 patients, consistent with our mouse data.
3% of the world population is homozygous for an APOE gene. APOE genes can also affect risks of Alzheimer’s disease, atherosclerosis and anti-tumor immunity.
Neutralizing antibodies against IL-1RA and a hyperphosphorylated IL-1RA isoform were observed in young male patients with biopsy-confirmed myocarditis after the receipt of SARS-CoV-2 mRNA vaccine.
9/21/22 Lancet: Outcomes at least 90 days since onset of myocarditis after mRNA COVID-19 vaccination in adolescents and young adults in the USA: a follow-up surveillance study https://buff.ly/3LxvJoy
mRNA Vaccine myocarditis, in 393 patients, age 12-29. Most recovered completely.
After >90 days:
81% fully recovered
16% improved
1% no change
9/21/22 via John Chi: Chinese scientists develop mask that detects COVID in the air https://buff.ly/3Smtrec
A sensor built into a mask was able to detect the COVID-19, H5N1 and H1N1 influenza viruses in the air within 10 minutes and send notifications to a device.
9/20/22 Proceedings of the National Academy of Sciences (PNAS):
Nanomolar inhibition of SARS-CoV-2 infection by an unmodified peptide targeting the prehairpin intermediate of the spike protein https://buff.ly/3BPBdI5
We discovered a simple peptide that inhibits infection by all major variants of SARS-CoV-2 with nanomolar efficacies.
Designed a peptide without the need for modifications such as lipidation or chemical stapling.
They have developed a special "hug molecule" [the Inhibitory Peptide] that keeps Covid from being able to do anything by tangling up its “grabby parts”.
9/20/22 TIME: Long COVID Experts and Advocates Say the Government Is Ignoring 'TheGreatest Mass-Disabling Event in Human History' https://buff.ly/3qU01sh
Vaccines and boosters protect against severe COVID and death. But, 1 in 5 people (20%) may get Long COVID after any COVID infection, even mild per CDC.
CDC guidance no longer recommends social distancing, mask-wearing, or screening tests for most people who don’t have symptoms, and unvaccinated people don’t need to quarantine if they’re exposed to the virus.
CDC should recommend people isolate more than 5 days if they are COVID positive.
In a 60 Minutes interview that aired Sept. 18, President Joe Biden said “the pandemic is over,” even though “we still have a problem with COVID.”
In addition to Long COVID risks, having COVID-19 also raises a person’s risk of developing chronic conditions including heart disease, asthma, and diabetes, according to CDC research. This will tax the healthcare system as well.
Long COVID can take many forms, including exhaustion, cognitive dysfunction, neurological issues, and chronic pain. There is no known cure for Long COVID, and the only way to prevent it is not to get infected at all.
Up to 4 million people in the U.S. are out of work because of Long COVID.
“Leaders have thrown their hands up in the air and basically said, ‘You do you,’” Kristin Urquiza.
In late 2020, Congress gave the NIH $1B to study long COVID.
The NIH’s cornerstone Long COVID research project aimed to enroll 40,000 people; as of August, it had enrolled only about 8,000. That’s in large part because of the complexity and scope of the trial, according to the NIH.
Long COVID will have a huge impact on the healthcare system, the economy, the work force, and the disability system for years to come.
“We’re in the middle of the greatest mass-disabling event in human history,”
9/18/22 President Biden says on 60 Minutes that the pandemic is over.
We will remain vulnerable if we pretend the pandemic is over.
Few Americans have gotten past booster shots. And declaring “the pandemic is over,” will not encourage Americans to get the new bivalent boosters.
Two reasons why the President’s statement is disconnected from the science.
Imprinting, meaning that after being exposed to an earlier strain of COVID-19, we do not mount as strong an immune response to new strains, thus giving the virus a further edge.
New variants, like BA.2.75.2, exhibit more evasion of our immune system than any prior version and may cause new waves.
We need nasal, oral or inhaled vaccines, rather than a shot as they are better at blocking infections and spread. Plus, people don’t mind a nasal spray as much as they do an injection.
Pan-sarbecoviruses nanoparticle vaccines would also be protective.
The US booster rate is only 33% despite the many studies showing benefit.
Boosters provide unequivocal benefit for protection from severe Covid and help reduce Long Covid (magnitude uncertain).
Disturbing trend of much lower antibody induction against Omicron variants compared to that mounted against the ancestral (original) strain. Perhaps because Omicron variants are less immunogenic or there is imprinting.
BA.2.75.2, a daughter of BA.2.75 ,has three new spike mutations that are concerning.
We can’t go on getting boosters every 4 to 6 months and the premise of an “annual” shot is that the virus exhibits seasonality like flu, which certainly isn’t the case. We need nasal vaccine boosters that stop infection.
9/18/22 NY Times: Potent New Covid Boosters Are Here. Will Weary Americans Bother?https://buff.ly/3Uw6M14
68% of Americans had 2 doses (fully vaccinated) with the original vaccines, but only a third have gotten any boosters despite them being available since Sept 2021.
Reasons why people may not get the bivalent booster include not being aware that there is a new booster for all people over 12 and older, concern about side effects (needing to miss work the next day because of fatigue), lack of perceived benefit and confusion with messaging, and thinking that the “pandemic is over” since the President said exactly that.
Still, 70,000 people are still getting sick every day and 400 people are dying each day from COVID.
Up-to-date recommendations that are updated regularly as new evidence emerges.
This updated (fifth) version contains 16 new recommendations for the rehabilitation of adults with post COVID-19 condition (PASC or Long COVID) (see Chapter 24) including:
New PSAs featuring Jeff Bridges, Kumail Nanjiani and Emily V. Gordon, and others
9/18/22 Evusheld
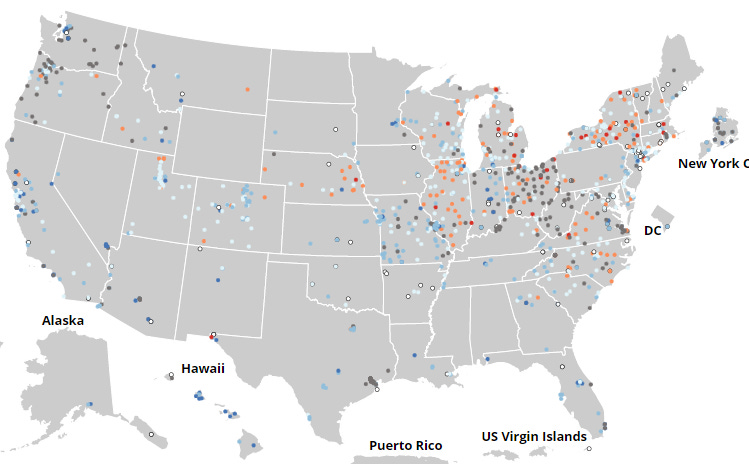
9/18/22 Twitter thread from wastewater virologist Marc Johnson on cryptic lineages found in some wastewater, probably from people with chronic SARS-CoV-2 infections, that are mutating and may predict that BQ.1.1 and BU.1 may be the new dominant VOCs in the next few months.
9/17/22 NEJM: A Bivalent Omicron (BA.1) Containing Booster Vaccine against Covid-19 https://buff.ly/3xsNUGo
Moderna bivalent booster (original virus mRNA + BA.1 mRNA) caused 2x increase of neutralizing antibodies against both BA.1 and BA.5. as compared to the Moderna monovalent original virus booster.
Vaccine effectiveness was not assessed in this study.
Even if just 5% fulfill criteria for Long COVID, that means 7.5 million individuals would be affected in the US. In comparison, each year in the US, approximately 1.8 million individuals are diagnosed with cancer and 1.5 million are diagnosed with diabetes.
It is impossible to overstate the challenge, complexity, and cost of responding to a new disease that will affect millions of individuals.
Author recommends a program like the National Vaccine Injury Compensation Program.
"Without a national program [for Long COVID], it is likely that individuals will not receive the care they need, disparities in care will inevitably develop, patients will be exposed to ineffective treatments, and staggering costs will be passed on to employers and state and federal governments. Only by creating a coordinated, national program, can we ensure an effective and equitable system of care for patients with long COVID."
Bivalent mRNA COVID-19 vaccines are now the recommended vaccines for use as a booster. Monovalent mRNA COVID-19 vaccines are no longer authorized for boosters.
Anyone aged 12 years and older who completed an initial COVID-19 primary dose or COVID-19 vaccine series should receive a bivalent booster two months following their last primary dose or monovalent booster (CDC COVID-19 Vaccination Schedule for Most People).
Individuals, including pregnant individuals, age 12 years and older who already received a monovalent COVID-19 booster should receive a bivalent booster at least 2 months after their monovalent booster.
9/14/22 Boston Globe: The latest COVID booster is recommended for pregnant women, so why don’t more of them know that? https://buff.ly/3DummnL
9/14/22 Mayo Clinic: Changes in Burnout and Satisfaction With Work-Life Integration (WLI) in Physicians Over the First 2 Years of the COVID-19 Pandemic https://buff.ly/3qT98cw
A dramatic increase in burnout and decrease in satisfaction with WLI occurred in US physicians between 2020 and 2021.
Emotional exhaustion scores increased 38.6%
Depersonalization scores increased 60.7%
Overall, 62.8% of physicians had at least one manifestation of burnout in 2021
30% satisfaction with WLI in 2020 compared to 46.1% in 2020.
Differences in mean depression scores were modest suggesting the increase in physician distress was overwhelmingly work-related.
Given the association of physician burnout with quality of care, turnover, and reductions in work effort, these findings have profound implications for the US healthcare system.
Thanks for reading Dr. Ruth’s Newsletter! Subscribe for free to receive new posts and support my work.