

COVID news 8/26/22

Hi all,
About 89% of COVID cases this week are from the BA.5 variant in the US. Overall, BA.4.6 cases do not appear to be outcompeting BA.5. One US region however, Region 7 (Iowa, Kansas, Missouri, Nebraska), has seen an increase of BA.4.6 cases from 8.7% of cases four weeks ago to 17.2% of cases this week. Hopefully, BA.4.6 will just be a small blip there.
Wastewater SARS-CoV-2 virus levels in the US are decreasing, albeit slowly. Virus levels have come down to about the same level that they were 2 weeks ago so there are still many people with BA.5 COVID in our neighborhoods. I wouldn't take off indoor masks just yet.
There was an outstanding article from the Brookings Institution this week showing the economic losses we face as a nation from Long COVID. About 16 million or 8% of working-age Americans (those aged 18 to 65) currently have long Covid. Of those, 2 to 4 million people (1.5 to 2% of the entire US civilian labor force) are disabled and unable to work which translates to $170-200 billion a year in lost wages alone. $170 billion represents nearly 1% of the total U.S. gross domestic product being lost. Billions of dollars more are lost from lower productivity and reduced hours for people with Long COVID who are able to work reduced schedules and from healthcare costs. Absent intervention, things will get worse. We need to make Long COVID a national priority and we need to put money into studying the causes of Long COVID and treatments that work.
On a positive note, Paxlovid's protects well against severe Omicron infections in high risk people including those over age 65. In Israel, Paxlovid reduced Omicron hospitalizations by 73% and deaths by 79% in people over age 65. It did not protect lower risk people aged 40 to 64 though. In Hong Kong, Paxlovid given to hospitalized patients during the Omicron BA.2 wave decreased death by 66%. And finally, in the US, outpatient vaccinated people who received Paxlovid for Omicron infections had decreased risks of emergency room visits, hospitalizations and death. Despite issues with Paxlovid rebound, the gnarly metallic taste, and the requirement to go off some medications during treatment, the data shows that it really is worth taking Paxlovid for higher risk people.
The bivalent booster containing mRNA to Omicron BA.5 and to the original Wuhan SARS-CoV-2 virus will be available soon after Labor Day. It is amazing that this vaccine was conceived and manufactured in about 2 months which demonstrates the promise of mRNA vaccine technology. But, this new booster does not come without some controversy. Eric Topol MD reviews this in his latest article "The imminent BA.5 vaccine booster". The bivalent BA.5 + original (WA1) virus vaccine has only been tested in mice (n=8) so far, and the mice did not get vaccinated with 3 or 4 doses of the original virus mRNA vaccine before they got the BA.5 bivalent vaccine. The mice did make good neutralizing antibodies with the new bivalent BA.5 vaccine.
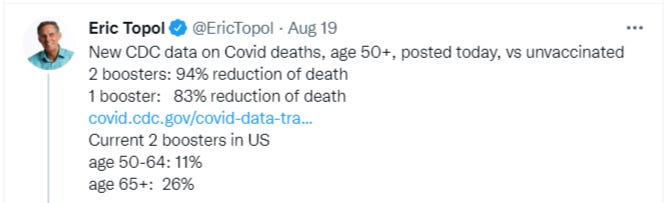
We do have human data for a BA.1 mRNA vaccine (monovalent and bivalent) in people, age 55+, with 3 prior doses of the original vaccine, indicating a good induction of neutralizing antibodies against BA.1 and a lower level of neutralization against BA.5. Some scientists question whether it would be better to give a monovalent booster of only BA.5 and not the original virus because of immune imprinting. Bob Wachter MD says that he will get the new bivalent BA.5 vaccine as soon as it becomes available, especially since he has not had a booster in many months. Others may wait. The US has a really poor record for people getting boosters despite many studies showing their benefit. Only 11% of people age 50-64 in the US have had the 4th dose booster and only 26% of Americans age 65+ have had their 4th dose booster. Akiko Iwasaki and Eric Topol had an op ed in Science magazine this week talking about how we should also be spending time and money on making nasal vaccine boosters which can stop the virus from entering the body with sterilizing immunity in the nose, mouth and throat.
Unless Congress approves more funding, the September vaccine booster will be the last free vaccine to be available to all Americans including those without health insurance. We also need Congress to approve funding to give PPE to healthcare workers and to pay for the manufacture and distribution of COVID tests. It seems like a good time to write to your representative asking the federal government to approve a funding package to pay for PPE, testing, vaccines and antiviral treatments for COVID for all Americans.
On one final note, Pfizer's 3 dose vaccine for the youngest children (6 months to age 5) shows a 73% vaccine efficiency against symptomatic Omicron infections. Only 6% of kids under 5 in the US have been vaccinated against COVID so far, but hopefully more parents will decide to vaccinate now that we have such promising data.
Have a good weekend,
Ruth Ann Crystal MD
Twitter: https://twitter.com/CatchTheBaby
Interesting non-COVID news:

8/22/22 Gothamist: Polio: How to find your long-lost vaccination records and other FAQs https://buff.ly/3KsyOGd
Very well written article on Polio and what you need to know.
8/22/22 Katelyn Jetelina: State of Affairs: COVID-19, MPX, and Polio https://buff.ly/3R3yeAu
COVID: BA.5 wave is starting to decrease but there is still spread. Almost 63,000 people worldwide and 15,000 Americans died during this wave.
Monkeypox (MPX): Some countries have successfully slowed the virus, particularly in the U.K., Germany, Canada, and Spain. Other countries show continued acceleration, like the U.S., Brazil, and Peru. 96.7% of transmission is in MSM.
Polio: London and New York continue to show community transmission of polio.
WHO recommends 95% of people to be vaccinated against polio to control the virus, but there are substantial pockets of unvaccinated people especially in NY state.
In NYC only 86% of children are fully vaccinated for polio, and in Rockland County only 37% of children are vaccinated.
If you and/or your child are fully vaccinated (3 to 4 doses), you’re fully protected against polio paralysis.
If you can’t remember if you were vaccinated or can’t find records, you should get vaccinated.
Antibody tests for polio are inaccurate because they cross react with some enterovirus antibodies.
Polio outbreak in 1950s. Kids in iron lungs 24/7 to stay alive:

COVID news:
World

United States

United States:

US cases (NY Times):

The number of US hospitalized patients with Covid is declining, down more than 6% from the recent peak in late July. But about half of states are still seeing increasing or flat hospitalization numbers, meaning they may not yet have turned the corner.
CDC variant proportions: https://covid.cdc.gov/covid-data-tracker/#variant-proportions


BA.4.6 is growing more quickly in only Region 7: Iowa, Kansas, Missouri, Nebraska
Wastewater virus levels:


Bay Area wastewater: https://soe-wbe-pilot.wl.r.appspot.com/charts


Outstanding article on Economic losses from Long COVID
8/25/22 Brookings Metro (Katie Bach): New data shows long Covid is keeping as many as 4 million people out of work https://buff.ly/3pJEced
Long Covid is a crisis.
Around 16 million or 8% of working-age Americans (those aged 18 to 65) currently have long Covid.
Of those, 2 to 4 million people (1.5 to 2% of the entire US civilian labor force) are disabled and unable to work which translates to $170-200 billion a year in lost wages alone.
$170 billion is nearly 1% of the total U.S. gross domestic product being lost.
Billions of dollars more are lost from lower productivity and to healthcare costs.
Absent intervention, things will get worse.
We must make Long COVID a national priority and must do studies and find treatments to prevent further loss.

8/25/22 NY Times Opinion by Zeynep Tufekci | If You’re Suffering After Being Sick With Covid, It’s Not Just in Your Head https://buff.ly/3AoyqDW
There are few treatments for Long COVID and lengthy delays to get into long Covid clinics.
Definitions of Long COVID are variable and this adds to the confusion.
In the UK, 2% of people said that Long COVID symptoms had affected their day-to-day lives, and 0.6% reported that their daily activities had been “limited a lot.”
For the United States, 0.6% of the population would mean about 2 million people potentially facing a debilitating condition, which is comparable to those expected to be diagnosed with cancer this year.
We need a National Institute for Postviral Conditions, similar to the National Cancer Institute, to oversee and integrate research.
Neither academia — prone to silos and drawn to work that leads to notable publications, which can leave important questions underexplored — nor the private sector — focused on profits — is up to the task alone.
8/25/22 NEJM: Paxlovid (Nirmatrelvir) Use and Severe Covid-19 Outcomes during the Omicron Surge https://buff.ly/3Aq4lUi
A marked reduction of hospitalization (73%) and death (79%) for Paxlovid in people age 65+ during the Omicron wave in Israel.
No evidence of benefit was found in younger adults age 40 to 64.
Hospitalization reduction data broken down by "immunity status" (vaccination, infection or both compared to no immunity) showing consistent benefit for age 65+, despite 8X higher event rate in those without immunity.



8/25/22 Lancet: Real-world effectiveness of early molnupiravir or nirmatrelvir–ritonavir in hospitalized patients with COVID-19 without supplemental oxygen requirement on admission during Hong Kong's Omicron BA.2 wave: a retrospective cohort study https://buff.ly/3AOYb1J
During the Omicron BA.2 wave in Hong Kong, among hospitalized patients without need for oxygen supplementation:
Paxlovid use showed a 66% reduction of death compared with matched controls.
Molnupiravir showed a 52% reduction of all-cause mortality compared to controls.
Oral antiviral recipients also had lower risks of the composite disease progression outcome, lower need for oxygen therapy and shorter time to achieve low viral burden than controls.
8/24/22 Reuters: U.S. first lady Jill Biden tests positive for rebound case of COVID-19 https://buff.ly/3QPWbf5
8/24/22 AP: Pfizer COVID shots appear 73% effective in children under 5 during the Omicron wave https://buff.ly/3Tmu7S0
Only about 6% of youngsters ages 6 months through 4 years had gotten at least one dose of a COVID-19 vaccine by mid-August.
8/24/22 Nature: Could tiny blood clots cause long COVID’s puzzling symptoms? https://buff.ly/3Tqv4ZQ
Scientists debate evidence for a microclot hypothesis that has some people pursuing potentially risky treatments. (Many scientists don’t believe this hypothesis.)

8/23/22 NY Times: Biden Administration Plans for New Booster Campaign Soon After Labor Day https://buff.ly/3wns6LO
The new bivalent (BA.5 + original virus spike) booster will be rolled out after Labor Day.
Pfizer BA.5 bivalent booster for everyone over age 12.
Moderna BA.5 bivalent vaccine will be for those 18 and older.
The US has a poor booster rate compared to many other countries. And, we are still averaging about 450 COVID deaths per day and this could rise in the coming months as people spend more time indoors.
Moderna and Pfizer have both submitted clinical data from human studies from a Omicron variant BA.1 bivalent vaccine, but the approval of the bivalent BA.5 vaccines will be based on data from mice studies.
The F.D.A. will not seek a recommendation from its outside advisory panel of experts, a step it usually takes before making new vaccines available.
8/24/22 Excellent article by Eric Topol MD: The imminent BA.5 vaccine booster https://buff.ly/3chQ7wK
The bivalent BA.5 + original (WA1) virus vaccine will be available soon but has only been tested in mice (n=8) so far.
The mice did not get vaccinated with 3 or 4 doses of the original virus mRNA vaccine before they got the BA.5 bivalent vaccine.
We have human data for a BA.1 mRNA vaccine (monovalent and bivalent) in people, age 55+, with 3 prior doses of the original vaccine, indicating a good induction of neutralizing antibodies against BA.1.
As expected, the BA.5 antibody response was not as high as for BA.1.
People have received 2 to 4 doses of the original (WA1) virus mRNA. If there is imprinting (original antigenic sin), it may be better to give a monovalent booster of just mRNA to BA.5 and not to the original virus (WA1).
Nasal vaccines would probably be better. Pan-coronavirus vaccines would be great too.
If people feel this booster was rushed or if people are concerned that we lack human data for the BA.5 vaccine specifically, it may cloud the public’s trust.
Only 32% of the US population have had any booster shot.
Despite 5 studies showing that the 4th dose of vaccine significantly reduced mortality compared with a 3rd shot, for cohorts as young as age 50+,
only 11% of people age 50-64 had 4th dose booster
26% of Americans 65+ had 4th dose booster.
This will be the last free vaccine distributed by the US government, as funds have run out and subsequent vaccines, boosters and drugs may cost people.
"It’s actually striking that in 2 months from the June 28th FDA meeting, there is a BA.5 vaccine booster made at scale. That is finally in keeping with all the excitement about the plasticity of the mRNA vaccine platform"
Eric Topol compares advantages/disadvantages of BA.5 bivalent vaccine approval without specific human studies:

8/23/22 MedRxiV: Neutralizing Antibody to Omicron BA.1, BA.2 and BA.5 in COVID-19 Patients https://buff.ly/3QNlJth
Live virus neutralization titers against WA1, Delta, BA.1, BA.2, and BA.5 in 187 hospitalized patients infected with Delta or Omicron strains.
Omicron patients made more antibodies against other Omicron subvariants than people infected with the Delta variant.
"It needs to be considered whether keeping the ancestral WA1 strain in the updated vaccine is of value or not."
8/23/22 PNAS: SARS-CoV-2 prefusion spike protein stabilized by six rather than two prolines is more potent for inducing antibodies that neutralize viral variants of concern https://buff.ly/3dWQJZn
COVID vaccines (Pfizer, Moderna, J&J) use a 2-Proline (2-P) substitution (also called preS-2P) to stabilize the spike protein.
This study in hamsters shows that HexaPro (6-P) leads to more robust antibody and cellular immunity and protects better against lung infection in hamsters than 2-P.
Since HexaPro is more immunogenic and protective, it may be better to use HexaPro in future SARS-CoV-2 vaccines.
8/21/22 LA Times Op-Ed by Eric Topol: We're starting to understand Long COVID. Next we can fight it https://buff.ly/3dGVC8G
Few therapies. Need for accelerating clinical trials of treatments is urgent.
“Our best chance to prevent long COVID is to not get COVID or to avoid getting it again. That’s why it’s vital to stay COVID-cautious now, and not capitulate to the notion that we should “live with COVID.”
8/21/22 Paxlovid during the Omicron wave: Oral Paxlovid (Nirmatrelvir and Ritonavir) in Non-hospitalized Vaccinated Patients with Covid-19 https://buff.ly/3T7NXQS
Retrospective analysis of Paxlovid in vaccinated high-risk outpatients shows a strong association between treatment and improved outcomes during the Omicron wave (Dec 2021 to April 2022).
Treatment with NMV-r in non-hospitalized vaccinated patients with Covid-19 was associated with a reduced likelihood of emergency room visits, hospitalization, or death.

8/21/22 Eric Topol and Akiko Iwasaki in Science: Operation Nasal Vaccine—Lightning speed to counter COVID-19 https://buff.ly/3R0KwtE
Intramuscular mRNA vaccines do not achieve respiratory mucosal immunity (in the lining of the nose and respiratory system) against Omicron in humans, but this has been shown to be possible with nasal vaccines in mice.
Nasal vaccines can achieve mucosal immunity which can block transmission of the SARS-CoV-2 virus. Mucosal immunity can complement the circulating immunity (T cells, B cells, antibodies) achieved with intramuscular COVID shots.
There are 12 nasal COVID vaccines that are in clinical development, and 4 have reached phase 3 randomized, placebo-controlled trials.
We need dedicated funding, priority, and breaking down of any regulatory hurdles for nasal vaccines. A new operation at lightning speed could help us get ahead of the virus and build on the initial success of COVID-19 vaccines.
8/20/22 Respiratory mucosal immunity against SARS-CoV-2 following mRNA vaccination https://buff.ly/3dJVipI
Mouse model shows nasal vaccine causes robust sterilizing immunity against SARS-CoV-2 entry into the respiratory tract cells.
The current COVID-19 vaccines are highly effective against severe disease development, likely through recruiting circulating B and T cell responses during re-infection, but offer limited protection against breakthrough infection, especially by Omicron sublineage.
Mucosal booster vaccination (nasal vaccine) is needed to establish robust sterilizing immunity in the respiratory tract against SARS-CoV-2, including infection by Omicron sublineage and future VOCs.

8/20/22 WSJ: U.S. Plans to Shift Bill for Covid Shots and Treatments to Insurers, Patients https://buff.ly/3Cr1OMw

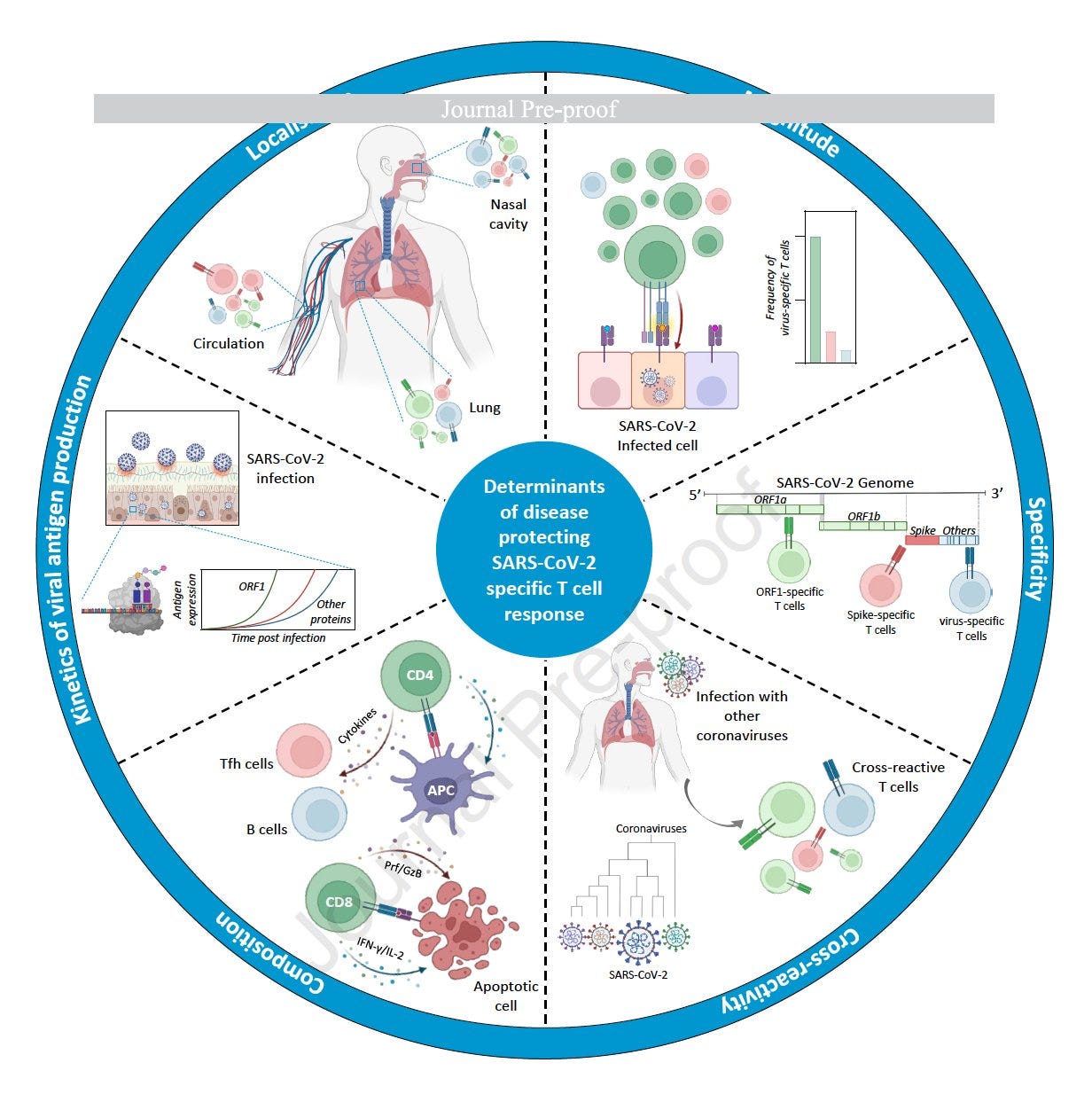
8/20/22 Cell: SARS-CoV-2-specific T cells in the changing landscape of the COVID-19 pandemic. https://buff.ly/3dOAYTY
Review of the T cell immune response from COVID vaccines, infections and the combination of both.
CDC: COVID-19 Cases and Deaths by Vaccination Status https://buff.ly/3p5JqCa
